February 24, 2015 · Comments Off on Mayra Arroyo: A Healthier and Happier Me

During the 4 weeks of class I learned so much. Not only anatomy, but I also learned a lot about my lifestyle choices and my study habits. Before taking this class, I had never really thought about how the choices I made affected my learning and my health. One clear example is the number of hours I sleep. I was used to sleeping at 12 am or later and snoozing for an hour every morning. After sleeping at 10 or 11 pm every night and waking up 6 or 7 am, I was able to see a difference in my energy levels through out the day. I did not have to take naps during the day and I also did not have to drink coffee to stay awake during the day. This allowed me to be extremely productive and be fully concentrated on what I was doing.
Another example is eating breakfast. I was used to waking up too late and not having enough time to go to breakfast. With my new sleeping habit I was able to go to breakfast every morning. I was the most proud of this new eating habit, not because I started it, but because I was able to continue it the whole month without quitting.
The last lifestyle change I made occurred the last week of class after watching “Sugar: The Bitter Truth”. I started to remove all juice from my meals. I have always known that soda is extremely bad for a person’s health, but I wrongly assumed that juice was not as bad. After watching this video I learned that juice is equally as harmful, and have stopped drinking it. Although I have not been prefect and have had juice, I am much more conscious about drinking water instead of juice at every meal. I also learned from this video that many of the things that we eat today contain fructose, even things that most people would not even think, such as baby formula. This was absolutely shocking and horrifying. I have started to look at the labels of food in hopes to reduce my consumption of fructose. I know these small changes will make a huge difference to health.
This class not only helped me become a healthier individual, but it has helped me become a better student. One way is that I am now a more organized. I have started to make lists in ranking of importance of things I need to accomplish each day. This has not only helped me be more organized, but it has also helped me to prioritize. This was significant for this class, because there was a lot of material. I had to focus on the most important ideas concepts, because it was impossible to study every single topic thoroughly. Although these changes may seem minor, they are not because this is the start I needed in order to become better and healthier student. I plan to continue these new habits during the spring semester and beyond.

Categories: Bi265j · Human Health
Tagged: Bi265j, Human Health, Mayra Arroyo
February 24, 2015 · Comments Off on Laurel Edington: MMSA Mentoring Session

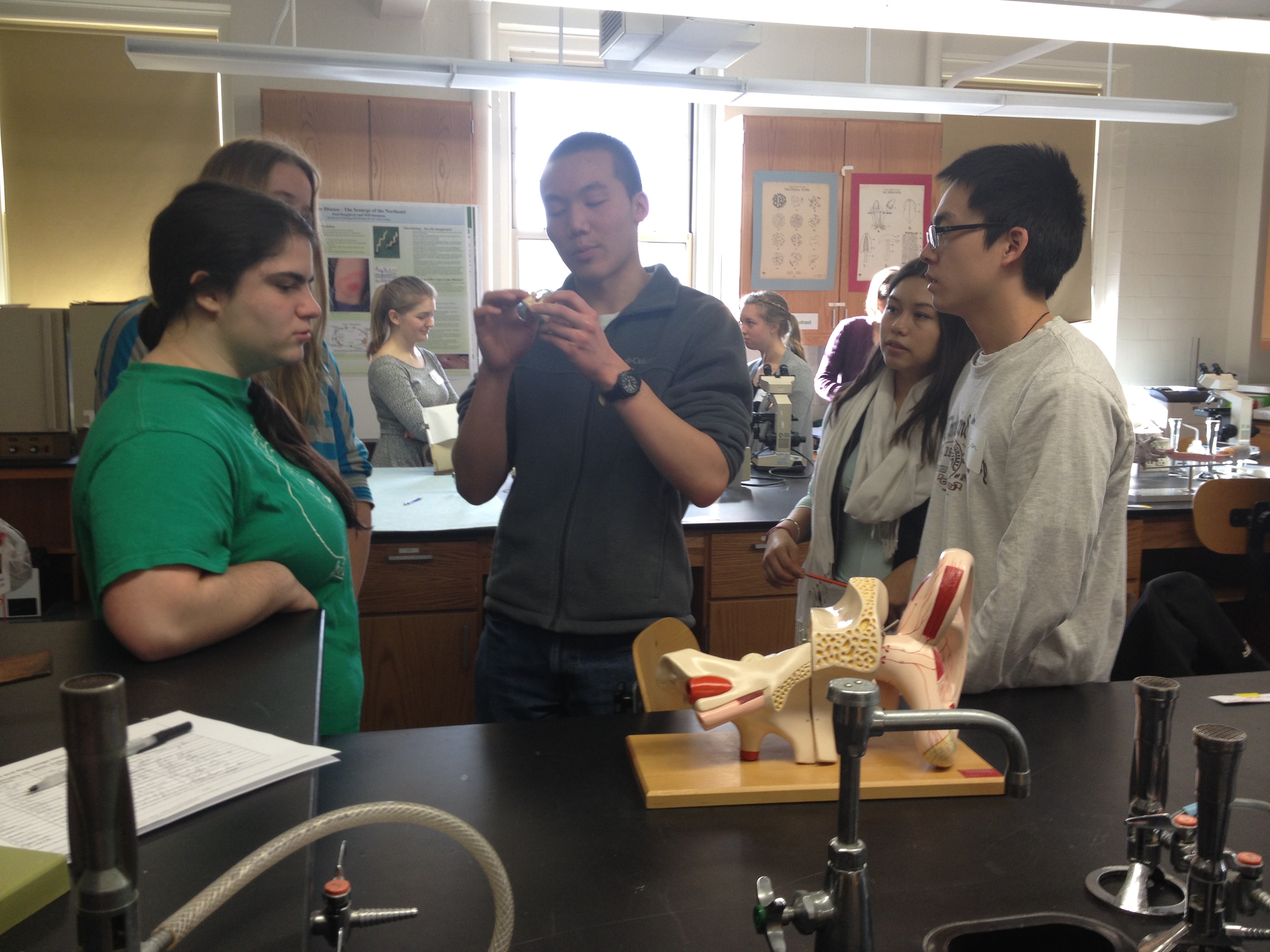
One of my favorite parts of this month was mentoring high school students involved in the Maine Math and Science Alliance. Each grand rounds group was paired with two high school students. The two girls my group worked with were named Shea-Lynn and Cierra. Shea is a home-schooled junior and Cierra is a sophomore at Dover-Foxcroft. The plan for the day was to show them around the lab, talk to them about anatomy and physiology, and help them come up with ideas for a science fair project.
Before the students arrived, we took our second lab practical and then walked around talking about the answers to the exam so that we could show the high school students what we have been learning over the past week.

 When they arrived and we were in our groups, we went through the entire exam with them. We all looked at the models and slides, explained the answers to each question, and explained the functions of each anatomical structure. This was great because it reinforced the material. Over the past few days I had been trying to memorize all of the structures of the neurons/spinal cord/brain, eyes and ears, and the cardiovascular system. By explaining the structures and functions to Shea and Cierra, it helped me to learn and understand the material even more.
When they arrived and we were in our groups, we went through the entire exam with them. We all looked at the models and slides, explained the answers to each question, and explained the functions of each anatomical structure. This was great because it reinforced the material. Over the past few days I had been trying to memorize all of the structures of the neurons/spinal cord/brain, eyes and ears, and the cardiovascular system. By explaining the structures and functions to Shea and Cierra, it helped me to learn and understand the material even more.

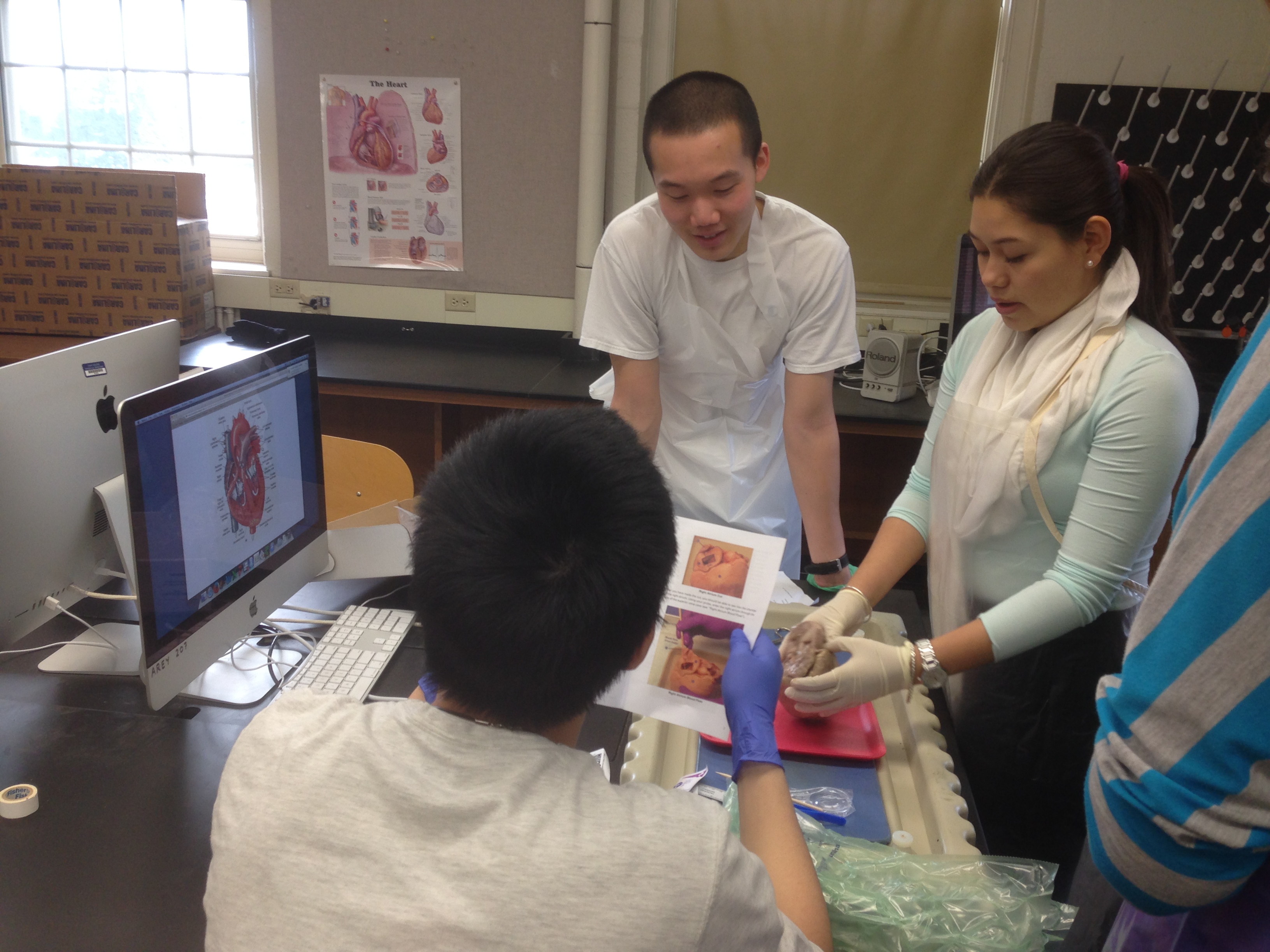
After the lab tour, each group dissected another pig heart since there were some hearts left over from the week before. I was really excited that I was able to be involved in a dissection on this day because I wasn’t able to be in class when we did the dissections the week before. Shea and Cierra, although a little timid at first, dove right in and were able to find the aortic and pulmonary valves very quickly. They did the of the dissection while we instructed and did a little demonstrating.


The last part of the day (after a quick lunch break) was used to help the students come up with topics for science fair projects based on anatomy and physiology. Cierra’s family owns a farm with over 50 beef cows so she wanted to do a project based on livestock. Together, we all came up with the idea of seeing how different types of food affect the growth of the cows. If she did this project, she was thinking of finding the mass and other size measurements for the cows of different ages and comparing the measurements between the cows that were fed hay and the cows that were fed grain. Shea was interested in determining if different emotions caused changes in blood pressure and heart rate. We talked about having people watch different videos that would cause them to experience different emotions and then she would take heart rate and blood pressure measurements before and after the videos to detect any changes. This day was very rewarding because we were able to reinforce what we have been learning, help high school students become excited about science, and we were able to have a great time.
Categories: MMSA Mentoring Session · Special Activities
Tagged: Dissection, High School, Laurel Edington, MMSA
February 24, 2015 · Comments Off on Ivan Yang: My experience in A&P

Even though I am a molecular biology major, I had not taken any biology courses in the fall semester, so my advisor highly recommended me to take a biology course for JanPlan. After checking the course listings for January, I decided on a whim to sign up for the Intro to Human Anatomy and Physiology course. Later that week, I met someone who had taken the course last January. She informed me that if I was to take BI265, I would have to be prepared to learn a lot in a small amount of time. There was a wealth of interesting knowledge to be gained from the course, but, she warned, if I was expecting to cruise through JanPlan, I should drop the course. Not sure if I should take her seriously or not, I laughed it off and didn’t think about her words much after that.


After the first week, I definitely knew that this class was not to be taken lightly. The first week was especially rough because of the flipped lecture setting. Not only did we have to study for daily quizzes and lab exams, but also we had to listen to lecture and lab podcasts for the following day’s lecture and lab sessions. I was completely unprepared, and I was forced to adjust my mentality, my study schedule, and my lifestyle habits. However, while there was a seemingly surreal amount of work involved in the course, the amount of material that I absorbed during the four weeks of JanPlan truly astounded me. In addition, after putting in maximal effort just to learn the basics of human anatomy and physiology, I gained deep respect and admiration for the structure and workings of the human body. I truly came to enjoy the class and the subject, and soon enough I found myself embracing Dr. K’s recommended healthy lifestyle habits.
Beyond learning material through lectures and labs and finding a healthy lifestyle balance between working and resting, I also had many opportunities to do things that I had never done before. For example, for the first time in my life, I had the opportunity to perform a wet dissection of a pig heart. Although I was confused at first due to initial difficulties in matching the neatly-drawn heart schematics in my mind with the real deal in my hands, I thoroughly enjoyed the experience of opening the heart with my own hands, placing my fingers through the valves and blood vessels to see where they connected, and seeing how the real tissues and membranes of the heart correlated with the models in our anatomy lab. In fact, I’m sure I would have enjoyed the experience even more if my partner and I had remembered that there were scalpels available for use in the dissection (we had to cut through a very thick ventricular wall with a very small pair of scissors – if you are taking the class and haven’t done the wet dissection yet, REMEMBER that there are scalpels available for use).

In sum, BI265 was a welcome and intellectually stimulating challenge. I absorbed a great deal of anatomy and physiology in the last four weeks, worked with wonderful classmates and a great professor, and learned about myself, my study and lifestyle habits, and stress management. I would recommend this class to anyone interested in thinking and in challenging his/her intellectual limits.

The blood vessel model – my best friend during the weekend before the second lab test.
Categories: Bi265j
Tagged: Bi265j, Dissection, Ivan Yang, Lab
February 24, 2015 · Comments Off on Ariel Oppong: A Memorable Aspect of Anatomy and Physiology- ART!

During the first week of class we made a trip to the Colby Art Musuem. Since the Art museum opened during the summer of 2013 I had only actually participated in one small tour. I feel like a version of myself enjoys art and objectively recognizes its value but a version of myself that is more present on campus does not really have the time or make the efforts to appreciate art. Thus, I was happy we went.
While we were there we completed a scavenger hunt that required our knowledge of different human muscles to find the art pieces that matched with eight different short stories and descriptions. We were allowed to work together or to work in groups of three or less.

After we completed the scavenger hunt we were asked to find a piece of artwork within the museum and to create our own question/description of the artwork with the central usage of a certain muscle being used by the characters or subjects in the artwork. For my question I decided to make focus on a 1997 piece of artwork called Leader by American artist, Betye Irene Saar. Born in Los Angeles, California in 1926, she has been known to incorporate collage and assemblages into statements of political and social protest.

In this picture, a strong woman is standing and maintaining the trunk of her body in a firm position. This position represents the woman’s strong presence in the family dynamic of families of this ancestry. Because of the importance of her stance as a symbol for other aspects of her womanhood, I decided to focus my piece on a large muscle that helps the main subject hold that stance: the gluteus Maximus.

The gluteus maximus is the largest and most superficial of the three-gluteal muscles (including the gluteus medius and the gluteus minimus). The gluteus maximus is proximally attached to the outer surface of the ilium and is distally attached to the superior and lateral surfaces of the greater trochanter of femur. As the largest and strongest muscle in the body, the gluteus maximus is both important in being responsible for the movement of the hip bone and thigh but in also in creating a shape to the human body and creating the appearance of hips. I really enjoyed learning more about Betye Saar, her work, and her work’s impact on general society. At first our student created scavenger hunt questions were supposed to be consolidated into a new list of synopsis for high school students to look at when they came to visit Colby early the following week. However, due to some logistical issue the students were not able to complete the scavenger hunt. Instead of completing a hunt, the high school students completed a heart dissection with us, The day prior to the students’ arrival on campus we had completed an almost trial run like heart dissections on our own in the lab. I enjoyed learning on my own and then showing the high school students different anatomical parts of the heart because it allowed me to see what aspects of the lessons before I was and was not retaining.
Categories: Bi265j · Special Activities
Tagged: Ariel Oppong, Art and Anatomy
February 24, 2015 · Comments Off on Calvin Robbins: My Celiac Disease Story

Every year, the BI 265 Jan Plan class holds student run Grand Rounds presentations. A Grand Round presentation is usually done by a doctor and patient (or actor) in front of other doctors to educate them of a surprising finding or elusive diagnosis, thereby helping the doctors in attendance better diagnose the problem in the future. This year a group presented about a man who had Celiac disease but presented as a cardiac patient (check out Ari, Danielle, and Laurel’s Grand Rounds presentation on celiac disease). It inspired me to tell my own story of being diagnosed with Celiac disease.
When I was 10 years old, I started to notice that when I coughed, there were small specks of blood in the mucous. Originally this was dismissed as an issue with dry air, as it was winter at the time, but as time passed, it was recognized as a larger problem.
The obvious assumption was a respiratory issue, so I had X-rays done which showed a very mild case of pneumonia. Soon the Pneumonia was treated but the blood in the mucous remained. Next came a series of blood tests, consultations, more blood tests, MRIs, X-rays, and still more blood tests, of which the only result was slight anemia. Guesses ranged from Acute Interstitial Pneumonia to tuberculosis to cancer, to a stomach ulcer, but every test came back negative. Doctors wanted to do a lung biopsy to check for AIP but my parents elected to wait for the Celiac results as a lung biopsy is invasive, carries a high risk of infection and would have had a long recovery period for an active 10 year old.
Finally, after about 3 months into an attempted diagnosis, a blood test was performed to test for Celiac Disease. The test was positive. An endoscopy was performed to verify Celiac Disease, as blood tests are not 100% accurate. The doctors discovered an abnormality in the small intestine: the villi were heavily flattened. Given this new insight, and after about a month of a gluten free diet, the blood speckling disappeared.
Celiac Disease is a genetic disease in which the body has an immune reaction to the presence of gluten, a protein found in wheat, rye, and barley. After blood testing it was found that my father and sister, who was asymptomatic, both have Celiac Disease, while my mother does not. From my family you might guess that it is recessive, but the actual inheritance mechanism is still unknown. Worldwide, it is estimated that about 1% of people are diagnosed with Celiac disease while most people with Celiac Disease actually remained undiagnosed.
Sticking with the theme of Grand Rounds, my case was actually presented as a Grand Rounds discussion by Dr. Andrew Filderman once the diagnosis was reached. It is thought that these types of atypical situations go undiagnosed or are improperly diagnosed most of the time they are presented, so spreading information about Celiac Disease is an important step in providing better care to patients.
Categories: Human Health
Tagged: Cal Robbins, Celiac Disease, Human Health
February 24, 2015 · Comments Off on Lauren Shirley: BI265J and Personal Health

One interesting aspect of BI265j was the emphasis that Dr. Klepach placed on personal health. On the first day of class, we were given sheets to track our sleep, exercise, stress, and eating habits. Initially, I was overwhelmed with the amount of information to absorb and the sheer scope of the class. Suddenly, I was trying to fit 4 hours of class, three hours of lecture online, sufficient exercise, three square meals and at least eight hours of sleep into a day, not to mention the actual studying part of learning for the class!
The first week was a bit rocky for me: trying to learn to use my time efficiently enough to get everything done while not succumbing to mental exhaustion at the amount of information I was trying to absorb was a challenge to say the least. However, switching back to a traditional classroom environment from the flipped environment was a lifesaver! By eliminating two hours of lecture from my homework load, I had sufficient time to study and exercise. I was able to go to the gym almost every day of the week (when I wasn’t fighting a flu).
I really enjoyed having part of the class be about maintaining our own personal health as a means to more effective learning. By placing an emphasis on exercise, I didn’t feel guilty leaving the library to go the gym for a study break. Instead, I embraced this new lifestyle opportunity and learned to play squash, something I had always wanted to do since coming to college, but had never been able to justify the time to do! Interestingly, I noticed that as I exercised more and put more of an emphasis on my own health rather than on numerical success in class, my stress decreased. I can’t say my quiz grades necessarily improved, but I felt like I was better able to absorb the material that was presented to me and was much happier while I was learning.
Also, by tracking my eating, I noticed that when my stress increased, my cravings for unhealthy foods increased as well. While I am not normally a person that eats a lot of baked goods or sugary foods, I definitely wanted them more when I didn’t exercise as much or get as much fresh air. This made me realize the importance of diet as a result of exercise.
Finally, I really enjoyed making sleep a priority during Jan Plan and received around eight hours of sleep every night on average with the exception of nights I was on duty as an EMT.
Thus, this class really taught me that my exercise habits impact both my stress and my diet, and that when I exercised less, other areas of my life would suffer. I was it metaphorically as similar to instructions for putting on an oxygen mask in a plane: Put on your own mask first before you help those around you. By focusing on my own health, effective learning and success will follow. Also, success is not defined just by numbers academically, but by your quality of life in general and how you feel.

Categories: Bi265j · Human Health
Tagged: Bi265j, Human Health, Lauren Shirley
February 24, 2015 · Comments Off on Danielle Levine: Heart Dissection and MMSA Visit
Danielle Levine (’15, Biology)

While taking Introduction to Anatomy and Physiology this JanPlan, I was given the opportunity to perform a wet dissection of a pig heart. Having learned about the surface and blood vessel structural features via the study of powerpoint slides, listening to class lectures, and studying plastic models, the wet dissection gave me the opportunity to view the anatomy learned in an actual heart. Studying a list of anatomical features and seeing pictures of them on paper is a very different experience from actually getting one’s hands “dirty” and exploring a real heart and seeing what those structures actually look like.
Besides being able to dissect the heart in lab, one of my favorite activities of the semester was when during the following week we dissected another pig heart with visiting high school students, and were able to show them everything we had learned about the heart the week before. On Martin Luther King Jr. Day, a number of high school students from different schools in Maine visited Colby for the day as part of a collaboration between the Maine Math and Science Alliance and the Colby Goldfarb Center; we were able to show the students around the lab and talk to them about anatomy and physiology, as well as help them with potential science fair project ideas.
That day, our class began with a lab practical that covered the eye, the ear, and the nervous and cardiovascular systems before the high school students arrived; after we finished the exam, we met the high school students who would be spending the day at Colby with us. Each lab group of Colby students partnered with two high school students, my group with Cierra, a sophomore from Dover-Foxcroft, and Shea-Lynn, a home schooled junior. After introducing ourselves, we took the high school students on a tour of our lab, showing them all the different models we use to help us learn about human anatomy. In addition, we went over with them the lab practical exam that we just took, explaining what the answers were (of course, we had an answer key, and we had gone over the answers in class after we had finished the exam), and the physiological significance of the various anatomical structures identified. This was a very enjoyable experience, as not only did it reinforce my knowledge of the material, but it also gave me the opportunity to share that knowledge with these students by teaching them a little bit of anatomy and physiology.

After the lab tour, we had enough pig hearts left over from the previous week, and so we were able to dissect another pig heart, this time letting the high school students perform the dissection while we helped and taught them about the different structures and features of the heart they were looking at – this teaching was reinforced by the use of pictures and models of the heart.
After successfully dissecting the heart and exploring its anatomic features (and after lunch), we talked about potential Maine Science Fair project ideas for Cierra and Shea-Lynn; they came up with some interesting topics such as the effect of emotions on heart rate and blood pressure. The day was very rewarding, as it gave me a feeling of competence in that I was able to teach others material I had learned in the course – not to mention, it was also a lot of fun!


Pictures of two of the heart models we used to study the cardiovascular system and teach the high school students with.
Categories: Lab · Special Activities
Tagged: Danielle Levine, Dissection, High School, MMSA
February 23, 2015 · Comments Off on Anonymous Student: Circumcision
Dr. Peter Millard recently came in for a talk about HIV and preventative measures in Africa, specifically discussing circumcision and its effects in nations severely affected by HIV within Africa. Dr. Millard actively supports circumcision and has equated the procedure with vaccination. There are serious issues with this claim. Circumcision and vaccines can not be equated. The amount of mental acrobatics it requires to compare a quick needle stick with a 15-minute unanesthetized surgical alteration of the genitals is ridiculous. Unlike vaccinations, botched circumcisions are common. Immunization prevents disease but circumcision is 100% chance of mutilation (Rebecca Grey). Vaccination also does not deprive an individual of any functional body parts. The foreskin is not just skin as Dr. Millard alluded. It is composed of mucous membrane, also called a prepuce, analogous to the eyelid or the inside of the mouth. People designated female at birth have a foreskin equivalent called the clitoral hood which evolved from the same tissue as the foreskin. Circumcision within US history has been tied to various fleeting reasons. The procedure was popularized by Dr. Kellogs during the Victorian era (the same person who co-invented corn flakes) to curb masturbation. He said:
“ The operation should be performed by a surgeon without administering an anæsthetic, as the brief pain attending the operation will have a salutary effect upon the mind, especially if it be connected with the idea of punishment.”
This masturbation hysteria was then replaced by fear of sexually transmitted infections followed by prostate cancer, and now urinary tract infections. Parents believe that circumcision helps with cleanliness, but they do not realize that there is something called a bath or a shower. Taddio et al. performed a meta-analysis observing the pain responses to subsequent vaccinations of circumcised infants and uncircumcised infants. They found that circumcised infants showed a stronger pain response than uncircumcised infants. The trauma of circumcision has lasting effects on these children. This logic of removing a functional body part to prevent disease is the same as selling a car to prevent a car accident (Men’s Health). Safe sex practices are what stops HIV transmission.
Dr. Millard mentioned that circumcision decreased transmission of HIV by 50-60%, but did not mention that a vaccine has essentially a 95% efficacy rate. Vaccination is about immunization, circumcision is not about immunization. The US has the highest HIV transmission of all the westernized countries and the highest circumcision rates. Evidence points to insufficient education about safe sex practices. In 1992, 410,00 cases of chlamydia was reported, 20 years later, 1.3 millions cases were reported. In 2000, there were 31,618 cases of syphilis, 10 years later, 45.834 cases were reported. It seems sex education among the general population is low. Instead, doctors are telling parents to circumcise their children instead of teaching children safe sex practices. Media now takes over where various sitcoms commonly have circumcision as a plot device which actively shames those who are not circumcised. Circumcision has become naturalized and not questioned.
Within the US, infant circumcision is still endorsed and is now supported by the WHO and the CDC which is backed by data from adult circumcisions in African countries performed on “consenting” adults. Infant circumcision forcefully separates the fused foreskin from the glans which results in the tearing of the synechia (the tissue that connects the foreskin to the glans) and keratinization of the affected areas. Circumcision is commonly used as treatment for phimosis, but infants can not get phimosis as their foreskins are not naturally retractable. The loss of protective mucosal membranes and various nerves denies the child of their own bodies and decisions. Before a child can even consent to having sex, they have their bodies permanently altered.
The voluntary medical male circumcision in African countries which is backed by the WHO is packaged with connecting men to health care, access to safe sex education, condoms, HIV testing, counselling services, and links to HIV care and treatment. These incentives behind the procedure drive safe sex practices which prevent HIV transmission. Proper habitual condom-use alone prevents HIV transmission by 95%. Circumcision can not be considered voluntary when access to safe sex tools and practices that prevent HIV are contingent upon this procedure. The institutionalized industry of circumcision is backed by ministers of health, policy makers, program managers, health care providers, and donors (e.g. PEPFAR and the Bill and Melinda Gates Foundation) who fund supporting programs. HIV transmission can also be transmitted through circumcision if the tools are not sterilized. Stopping circumcision means stopping access to health care. Of course the HIV transmission rates decrease when patients are educated on safer sex practices. The studies done in Africa were decided to be unethical after two years, but did not mention the unethical issues behind the actual circumcision itself. Long term follow-up should be required for these patients.
The exporting of circumcision results in growing acceptance of this procedure “in communities, among men and their partners, adolescents and parents” (WHO). Although studies have been done on adult men, the WHO supports influence on adolescents who are not given complete informed consent especially when their parents and the institutions manipulating the conditions favor circumcision. Many nations curtail to the US when it comes to health policies. Circumcision has become tool to normalize and impose Western standards of bodies on peoples that can not fully consent.
Circumcision in African countries are funded by western imperialism which exports this practice outside to different nations only to import the “results” back into their own countries to continue non-consensual practice of genital mutilation. This dangerous cycle impacts bodies in very specific ways to normalize cognitive dissonance. Babies do not have consent over circumcision. Continued practice of circumcision normalizes a dangerous environment for those designated male at birth. Why must this procedure be made by doctors paid to cut off foreskin? The infant has no agency over their bodies. Circumcision is a practice that attempts to manage disease, but does not answer the question of how disease can best be managed. Cultural bias coming from Dr. Millard reflects normative nontherapeutic circumcision sentiments within the US.
Sources
- https://www.psychologytoday.com/blog/moral-landscapes/201109/more-circumcision-myths-you-may-believe-hygiene-and-stds
- http://www.ncbi.nlm.nih.gov/pubmed/9057731
- http://pediatrics.aappublications.org/content/early/2013/03/12/peds.2012-2896.full.pdf
- http://www.parenting.com/blogs/pop-culture/shawn-parenting/circumcision-vaccine-against-bad-parenting
- http://www.cbsnews.com/news/circumcision-rates-declining-health-risks-rising-study-says/
- http://www.who.int/hiv/topics/malecircumcision/male-circumcision-info-2014/en/
Categories: Guest Speakers · Human Health
Tagged: Circumcision, Guest Speaker, Human Health, Peter Millard
February 23, 2015 · Comments Off on Rachel Bird: The End of My Gymnastics Career

I used to be squeamish. I was the kid who’d cover their face during movie fight scenes and feel nauseous at the sight of a bloody hangnail. Then I hurt myself — badly — during gymnastics practice, and I realized that as queasy my innards made me, it was worth it to understand them. When I fell on the trampoline during a routine in April 2012, I shattered my left radius and ulna. The repeated bouncing after the initial fall damaged the soft tissue and left the bones in a compound fracture, puncturing my skin halfway up the forearm. Although the initial reconstructive surgeries were able to salvage some of the bone and repair the structure of my arm, the massive soft tissue damage made my arm swell under the surgical dressings. My fingers grew so puffy with edema that they pressed together, despite the dressing that kept them spread as wide as physically possible. My elbow swelled to the size of my knee, and the staples holding the skin on the inner side of my forearm split open and the wound started oozing.

Eventually, the doctors diagnosed me with compartment syndrome, a condition that is common in crush injuries, but not frequently found in the type of break I had. Because of all the damage to the muscle tissue, my arm had swelled so much that the blood vessels were squeezed almost shut, preventing oxygen from getting to the nerves and muscles in my hand. Unfortunately, by the time I was diagnosed with compartment syndrome, the damage had already been done. The typical treatment for compartment syndrome is a WoundVac, which is essentially a vacuum that attaches onto an opening in the dermis and sucks out all the excess fluid before it can cause a problem. However, by the time the nurses had removed my surgical wraps and determined the cause of the swelling and burning sensation in my arm, the swelling had already begun to subside. Initially, the doctors believed that the nerves would be able to regrow, and most of the damage could heal on its own. However, after two months of daily occupational and physical therapy, I still had no sensation in my wrist, palm, or fingers. Even worse, the build-up scar tissue had cemented my fingers into a fist, and I only had roughly 15 degrees of mobility in my elbow and even fewer in my wrist. My hand was so stuck that I was unable to open my hand to trim my fingernails, so they were starting to grow into the skin on my palm. I didn’t even notice until it started bleeding, because I had no functioning pain nerves in my hand. I also had no proprioception, so when I wasn’t looking at my hand, I would have no idea where it was. This led to some funny encounters, because I would all-to-frequently end up with my hand in my food, or touching a stranger’ back!

After visits to numerous specialists, Dr. Barth, an orthopedic surgeon who specialized in hand and foot injuries suggested an unusual fix. He planned to surgically open up my forearm and scrape the scar tissue off of the joints and tendons in my hand. He would also remove the dead muscle tissue, but leave the muscle bellies (the central portion of a muscle), in the hope that the few remaining muscle fibers would be able to grow. Hopefully, without all the scar tissue blocking blood flow, some of the nerves in my arm would be able to grow back.
Luckily, the surgery was mostly successful, and I was able to open my hand. Less than two weeks after I was discharged from the hospital, I was able to feel deep pressure in my wrist and in parts of my palm! Nerves regrow at approximately five millimeters per day for larger nerves, so as my median nerve inched up my palm, my occupational therapist could track its growth with touch charts and a photocopy of an anatomy textbook. However, so much muscle and tendon was removed, that even though I was slowly able to feel the proximal areas of my fingers, I didn’t have the strength to move them. My arm was so weak that I had to wear a sling for most of the day because I couldn’t support my hand. Even worse, because I couldn’t feel scratches or cuts, two small paper cuts on my fingers got infected.
Dr. Barth proposed another surgery. He wanted to transfer a tendon from my upper arm into my forearm, in the hopes that I could “retrain” my brain to use one tendon for a different purpose. The surgery transferred the brachioradialis tendon and attached it to my extensor pollicis brevis, so when I wanted to move the distal joint of my thumb, I would have to think about bending my elbow. He also transferred the flexor carpi radialis and attached it to the flexor digitorum superficialis, so when I wanted curl or flex my fingers, I would use the muscle that had previously bent my wrist.

Although the process of recovering from this surgery and relearning how to use my hand to nearly two years, I am now able to type this paper using both hands (admittedly, it’s kind of awkward)! Unfortunately, having blood flow cut off to my nerves for so long had left me with permanent nerve damage, and I deal with chronic nerve pain and pretty limited strength and mobility. However, I can tie my shoes, dress myself and function in a classroom setting in ways that I couldn’t have dreamed of in the months following my accident, and I am so thankful to modern medicine for that!

Categories: Human Health · Personal Story
Tagged: Human Health, Personal Story, Rachel Bird
February 23, 2015 · Comments Off on Rachel Bird: My Concussion
Let me preface this by saying that I do not know how to ski. However, I’m a decent snowboarder, and I (mistakenly) thought that the two skills were relatively similar. Apparently I’m quite incorrect. The result is that this entire blog post is hearsay. I have absolutely no memory from Saturday, January 17 until Monday, January 19. According to my friends, on Sunday morning, we all got up early to drive up to Sugarloaf mountain to enjoy Colby Ski Weekend, with discounted lift tickets. The morning skiing was decent, but crowded. I was slowly (but surely) figuring out how to ski, and when we stopped for lunch I was feeling pretty confident. After a few successful runs in the afternoon, it was starting to rain, and the slopes had become slick and icy. We decided to do one last run and then head home. Our group got split up on one of the turns, and I ended up going ahead. When I hit a particularly icy patch, my right ski slipped out from under me and I rolled down a hill. I ended up at a fork in the trail and I went right, following a skier in black who I assumed was my friend. At the next fork in the trail, the only options were two different black diamonds, and the woman I had been following was clearly not a fellow novice skier! I reluctantly chose the path to the right and crossed my fingers. Initially, I was doing fine, slaloming side to side and avoiding the smooth icy patches in the center. Then I came on a steep slope and started to lose control. I tried to slow down, but the rain and melting ice didn’t offer any traction for my rental skis. I careened off the trail and down a hill into the woods, banging my skin on a branch and knocking the base of my head against a tree stump. I blacked out.
I woke to an old man in a green jacket poking me with his ski pole, “Are you okay, sweetheart?”
“Yeah, I’m fine, just give me a second.”
I crawled out of the woods and adjusted my goggles on my too-big rental helmet. I clamped my skis back on and gingerly slid the rest of the way down the mountain to the lodge. I mechanically returned my skis, boots, and helmet, and returned to our picnic table to change into dry clothes. I felt fine — a little drained, but that’s understandable after a long day at the mountain. As we waited for the shuttle to take us back to the parking lot, sleet and rain pelted down. The shuttle finally showed up, but on the way to the parking lot, my head started to pound. I blinked the snow out of my eyes, but my vision stayed blurry.
“Hey Chris — I think I’m seeing double.”
My boyfriend’s face swam in front of me, his mouth splitting into two identical sets of lips and then merging back into one.
“Do you feel okay?” Michaela’s voice piped up from my periphery, her head smearing into an unidentifiable mass.
“Um… I don’t know. I think I hit my head pretty hard when I fell.”
“We’ll get you to the health center when we get back to campus.”
“Ok.”
The shuttle pulled up to the parking lot, and I slouched into the backseat of Tenzin’s car. The sleet kept pouring down as we inched down the steep road. I slumped over on Chris’ shoulder, but he kept shaking me awake.
“Rachel, I really don’t think you should go to sleep yet, you might have a concussion.”
Then the car swerved and Tenzon overcorrected and the wheels slid and the road curved and we were in a snow bank. My head whipped forward and hit the seat in front of me with a resounding thump. Tenzin and Katie climbed out the front doors to survey the damage. The car was fine, but we were clearly stuck in the snow on the side of the road. Luckily, an ambulance happened to be passing by and the EMTs pulled over to see how we were doing.
“We’re all fine, but our friend is in the back seat, and we think she’s got a concussion.”
I crawled out of the back window, and stumbled over the the ambulance. The EMTs chattered between themselves, and apparently reached some consensus, because I was loaded into the back of the ambulance and barraged with questions.
“What year is it? What’s your name? Who is the president? Where do you live? Do you know your address? Are you taking any medicines?”
“Um. I don’t remember… I’m really sorry. I don’t know… uh… I don’t remember.”
Everything was fuzzy as the EMTs started an IV, and I dry-heaved into a plastic bucket.
“Zofran for the nausea and fluids for dehydration.”
I slumped onto the stretcher and blinked in time with my head’s pounding. Somehow I made it to Farmington Hospital and into a hospital bed, but I was too busy focusing on the peculiar way my forehead was pulsing. More nurses with more questions that I couldn’t quite conjure the answers to, more bright lights and beeping noises that made my head pound, more medical terminology that I was sure I had heard before, but I couldn’t quite place. The tall doctor called for a CAT scan, but I needed to give a urine sample first to prove I wasn’t pregnant, and my head hurt too much to get up and use the bathroom. But I gave the sample, and got the scan, and went back into my hospital bed, and tried not to fall asleep with my eyes open, because I was so damn tired. Hours or maybe seconds passed and the tall doctor sauntered back into the room. My boyfriend jumped up and began badgering him with questions. I took the opportunity to promptly fall asleep while sitting up.
“No internal hemorrhaging, which is good, but she’s got a pretty severe concussion…”
The doctor’s voice trailed off into technicalities, but I was already fast asleep.
Categories: Human Health
Tagged: Concussion, Rachel Bird
February 23, 2015 · Comments Off on Laurel Edington: My Experience in Bi265j
This January, I was given the opportunity to take the Introduction to Human Anatomy and Physiology janplan class. I’m a senior biology major and have finished all of my major requirements so I didn’t need to take this class, but I’m interested in the material and figured that it would be helpful to be at least familiar with human A&P when I’m eventually in medical school.
During the first week of class, I thought that the workload was too much and I considered dropping the class. Throughout this week, Dr. Klepach kept reinforcing that the first week was the hardest and that he really just wanted us to learn how to deal with a heavy workload and learn the material while still eating three meals a day, working out each week, getting eight hours of sleep each night, and keeping our stress level low. At first, I thought this was insane. How was I possibly supposed to learn all of these bones and muscles and not be stressed?! However, throughout the month, I realized that this was possible. The way the class was set up allowed work to be spread out so that we continued to reinforce the material through quizzes and preparing for lecture and class. By doing this, studying for a bigger exam or working on a bigger project ended up not being as stressful or time consuming as I imagined it would be.
The following weeks were still intense but were more manageable. Although we had quizzes before most lectures, another lab practical, a grand rounds presentation, and a few lab assignments left, Dr. Klepach’s advice of studying to learn the material and not for the grade really helped to make the class less daunting. As a premed student, I’m used to focusing only on the grades I receive and my GPA, but this class made me focus on actually knowing the material. Out of all of the classes I’ve taken at Colby, I’ve learned the most in this class. I don’t think this is because of the sheer amount of material thrown at us and if only a little stuck with us, it would be more information than some classes teach in a semester, but rather that I was actually working to learn the information and not just studying so that I could remember the material only in order to do well on the next test.
I highly recommend this class. I think it’s a great class for any premed student, any biology major, as well as any student who is just interested in anatomy and physiology. We were given so many interesting opportunities that no other class really offers. I can’t think of another biology class that performs any sort of dissection, that teaches the important skill of giving a grand rounds presentation, or that has lectures from specialists such as Dr. Zak Nashed and Dr. Peter Millard. During this month, we learned so much and we only just scratched the surface. I found this class so fascinating and wish that it could have been a semester long, or even a year long, course.
Categories: Bi265j
Tagged: Bi265j, Laurel Edington
February 23, 2015 · Comments Off on Chris Lee: What I Gained From BI265

This year I decided to sign up for BI265 (Introduction to Anatomy and Physiology) for my Jan Plan course. Going into it, I had no idea what to expect. I knew from my experiences with high school anatomy that it would require a lot of memorization. Given the fact that the class would only last for a month, I also expected the class to move at a very rapid pace. With these thoughts in mind, I walked into the classroom on the first day, ready to begin my second Jan Plan at Colby.

On the first day, Dr. Klepach told us that one of his goals in the course was to teach us to maintain healthy lifestyles, despite the rigorous nature of his class. According to him, this would be an important lesson to learn, especially for those of us who entered the health professions field. Maintaining a healthy lifestyle, especially while taking a course like BI265 at first seemed impossible. We were exposed to a lot of information each class and it was not uncommon for us to have quizzes the day after we were introduced to new material. During the first week, I spent nearly all my time outside of class in the library going over lecture notes and stressing over whether or not I had studied enough. I wondered how it was possible to fit in time for sleep, activities outside class, and three meals a day without stressing out. As it turned out, it was possible to achieve all three of these things and succeed in the class. All it took was some self-reflection and time management.

Self-reflection is an all-around good skill to have. It lets you evaluate where you are in the process of trying to accomplish something and lets you see where your strengths and weaknesses lie. In my case, self-reflection let me see a major weakness in my approach toward the class: my study habits. Usually, my approach to studying would be to re-read my notes until the information sank into my head. For a Jan Plan course, this is inefficient because time is very limited. After an unsuccessful performance on the first lab exam, I sat down and thought about how I was studying. I concluded that I needed to implement a more active style of learning. For instance, when studying the different parts of the eye, heart, and ear, I looked at anatomical models of these organs in addition to looking at the diagrams in my notes. Our lab exams asked us to identify structures on anatomical models, which was why it was more beneficial to study the models in conjunction with diagrams. Being able to self-reflect on my performance in the course helped me make the necessary changes to how I approached the material and improve my performance.
In addition to self-reflection, time management was another important skill that helped me get through BI265. In order to fit in time for sleep and other activities outside of class, I had to stay focused and be more efficient when it came time to work. Doing this allowed me to be productive while allowing for more time to enjoy myself outside of class. A technique I used to help with time management was setting up an organized schedule. Through this method, I was able to see when I could devote time to study, keep track of deadlines, and plan ahead. I attribute my decrease in stress levels to an improvement in my time management skills. Being more organized helped me get more done sooner so that I was not left with an overwhelming amount of work in the wake of an imminent deadline (which is very stressful situation). While I learned a lot about the cardiovascular, skeletal, digestive, and other body systems in BI265, I also learned the importance of self-reflection and time management. I have no doubt that these two skills will be beneficial to me for the rest of my college career and ultimately the rest of my life.
Categories: Bi265j · Human Health
Tagged: Bi265j, Chris Lee
February 23, 2015 · Comments Off on Chris Lee: Dissecting a Sheep Heart
I cut the plastic bag open and was immediately hit with a strong odor. Inside the bag was a sheep’s heart, sitting in a pool of preservative chemicals. Immediately after taking the heart out, I went over to the sink to rinse off the chemicals. I could tell that this was going to be a messy lab. Still, I was excited to do a sheep heart dissection because it was an opportunity for me to see a real heart. For about a week, I had been studying diagrams and models of hearts, but not a real version of the organ itself. The anatomical models we used were helpful in learning where structures of the heart are located, but nothing beats seeing the real thing.
After washing the heart, my lab partner and I located its apex (tip) and figured out where the left and right sides were. It was immediately apparent that not all the structures were intact which was unfortunate (both the inferior and superior vena cava had been cut off). However, we discovered a well-preserved depression known as the foramen ovalis behind the right ventricle that had not been damaged in the preservation process of the heart. The foramen ovalis marks the former sport of the foramen ovale, a hole in the pig fetus’s that helps with blood circulation. After the pig’s birth, the hole is sealed, leaving behind the foramen ovalis.

Next, we started cutting the heart open. Cutting through the walls of the heart was difficult. The heart’s function, to pump blood throughout the body, requires it to be a tough, durable organ and I was reminded of this as my lab partner and I tried to cut through its walls. Pulling apart an incision on the right side revealed a small chamber with a hole in its lower end covered by three flaps. This was the tricuspid valve, the covering between the hole connecting the right ventricle and right atrium. I stuck my fingers through the valve, pushing my way past the three flaps into the larger space known as the right ventricle and felt around. Brushing against my fingers were the stringy cordae tendinae that connected the flaps of the tricuspid valves to the papillary muscles.
Over on the left side of the heart, we saw structures such as the left atrium, bicuspid valve, and the left ventricle. While making a cut on the left side of the heart, I immediately noticed how much thicker the muscular walls were on this side. Something that occurred to me during this dissection that I never really thought about before was how the heart’s form fit its function. Its thick, muscular walls (particularly on the left side) gave it the necessary power to pump blood to different parts of the body. The cordae tendinae, though somewhat thin and stringy, still felt strong and durable, which was necessary for them to be able to keep the bicuspid and tricuspid valves shut. Even the layout of the heart itself is essential to its function. It contains four chambers linked by a straightforward path that enables deoxygenated blood to enter, get pumped to the lungs to pick up oxygen, return, and then get pumped to other parts of the body. The sheep’s heart dissection was definitely my favorite activity from anatomy class. I enjoyed the hands-on aspect of it and being able to explore the layout and structure of a real heart.



Categories: Bi265j · Lab
Tagged: Chris Lee, Dissection
February 23, 2015 · Comments Off on Laurel Edington: Grand Rounds – Celiac Disease
During the last week of class, we presented our grand rounds talks that we’ve been working on all semester. This was a great experience because it allowed us to practice giving a grand rounds lecture, which is a common presentation in the medical community. Each group of three picked a topic, which could be a case study or an overview of a disease or medical treatment, and then presented as if they were doctors talking about an interesting patient, new procedure that they’re performing, etc.
This year, the weather didn’t exactly cooperate with us. We were supposed to have a practice session during class on Tuesday and then go to Augusta to present our talks along with Kents Hill students at Maine General. Because of the snow day and horrible driving conditions, neither of these events happened and we had to present our final product with little group practice. Thankfully, my group was able to practice together before the weather was too bad, but practicing during class and at Maine General would have been helpful.
My group decided to present a case study on a 42 year old man with chest and abdominal pain. We found this study through the New England Journal of Medicine and it was used as a hugely teaching moment instead of a typical grand rounds talk. In this case study, the man’s symptoms were textbook for celiac disease but physicians performed a number of tests, including an invasive and non-diagnostic procedure, before even thinking of the possibility of celiac disease. This case study was not used to teach medical students and medical professionals about a rare disease or an interesting case, it was used to enforce the fact that celiac disease is becoming increasingly common and physicians need to be aware of it and perform the simple diagnostic blood test for the disease when a patient comes in presenting characteristic symptoms.
Through this presentation, we learned the difference between celiac disease and non-celiac gluten sensitivity. With celiac disease, there is damage to the intestines and an IgA tissue transglutaminase and IgA endomysial antibody tests can be performed to diagnose the condition, this is not the case with a gluten sensitivity. Both conditions, however, are treated with a strict gluten-free diet. This is becoming a popular new diet in people who don’t suffer from celiac disease or non-celiac gluten sensitivity. People who are using this fad diet and who don’t have celiac disease or a gluten intolerance are at risk for developing new gastrointestingal problems.
This project was a great way to expose us to this sort of presentation since the majority of the class is interested in the medical profession and grand rounds are a common occurrence. This was an especially interesting experience because we were able to present in front of nurses and doctors, which made the experience that much more real. It also reinforced the material we had learned throughout the class because we had to explain the disease based on the anatomy and physiology. I’ve been to multiple grand rounds during my summer internships and I never thought that I would be able to understand a case as well as those doctors, but this experience showed me that I am more than capable and therefore, was an awesome experience.
https://www.youtube.com/watch?v=DiKDOyG6Olg
Categories: Grand Rounds
Tagged: Celiac Disease, Grand Rounds, Laurel Edington
February 23, 2015 · Comments Off on Ivan Yang: Musings on the Fetus vs. Mother Battle
One of the best yet most challenging parts of this course is the sheer volume of knowledge that can be gained in these four weeks. I learned a spectacular amount of information about the human body during the course, giving me a greater appreciation for the ingenuity of evolution and the delicate intricacy of the body’s structures and mechanisms. In addition, Dr. K has a knack for sprinkling little bits of knowledge throughout his lectures that, when given time to soak in, can stimulate a great deal of critical thinking.
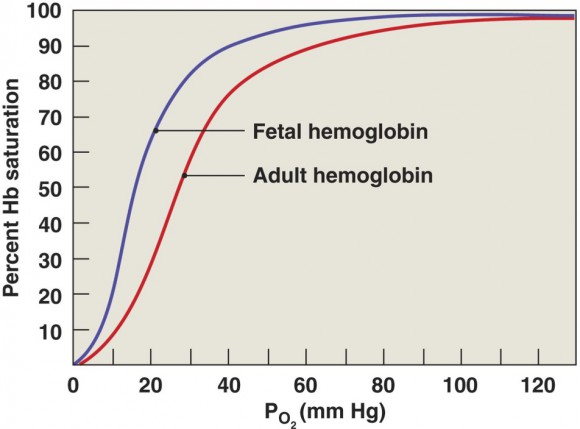
For example, when Dr. K lectured on the respiratory system, he briefly mentioned that fetal hemoglobin has higher oxygen saturation than adult hemoglobin does at the same oxygen levels. While this assertion can be explained by the fact that the fetus has higher demand for oxygen and must compete for oxygen in slightly deoxygenated blood, it reminded me of an article I read in a previous biology class on imprinted genes.
Imprinted genes are genes which are “marked” by the maternal or paternal parent and which are expressed over other versions of the same gene. Mechanisms of imprinted gene expression and evolutionary reasons for their existence are mostly obscure due to their relatively recent discovery. In fact, the existence of imprinted genes was only verified through cloning experiments in the late 80s. Scientists attempting to create a uniparental mouse (a mouse with two paternal or two maternal sets of DNA) found that it was impossible to create a fully-developed uniparental embryo. When the embryo was created from two maternal sets of DNA, its cells were properly organized, but the placenta was insufficient. When the embryo was created from two paternal sets of DNA, it was able to form a very healthy placenta, but the fetus itself was a disorganized mass of cells.
These results flew in the face of Mendelian genetics, which suggested that genes are merely strands of information with no history of origin. To the contrary, genes do, in a sense, remember their parental origins. The studies in the 80s suggested that the expression of certain genes in the paternal genome is responsible for making the placenta, while the expression of certain genes in the maternal genome is responsible for organizing the embryo. One of the first explanations posited that the placenta should be thought of not as a maternal organ designed to support the fetus, but rather as a fetal organ designed to parasitize the mother. While the mother and the fetus both have the common purpose of perpetuating the continued survival of the fetus, they disagree over how much of the mother’s resources should be dedicated to the fetus. In a sense, maternal genes are “selfish” and only the genes necessary to organize the fetus are expressed. Hence, the uniparental mouse embryos made of two maternal sets of DNA were unable to create a sufficient placenta.
This competition for resources between the fetus and the mother, clearly observable through research on imprinted genes, is strikingly similar to the competition for oxygen between the fetus and the mother. As previously mentioned, fetal hemoglobin has a higher oxygen affinity than adult hemoglobin does. To ensure its own survival, it is entirely conceivable that the fetus robs oxygen from the mother’s bloodstream. Perhaps this is but another example of a battle of wills between the fetus and the mother.
Categories: Human Health
Tagged: Human Health, Ivan Yang
February 23, 2015 · Comments Off on Calvin Robbins: Lyme’s Disease
In the last decade, occurrences of Lyme Disease in Maine have been increasing at shocking rates. Colby is a school with a very outdoor-oriented student body, so information regarding Lyme Disease and its effects on the human body is something that everybody should take the time to look at.
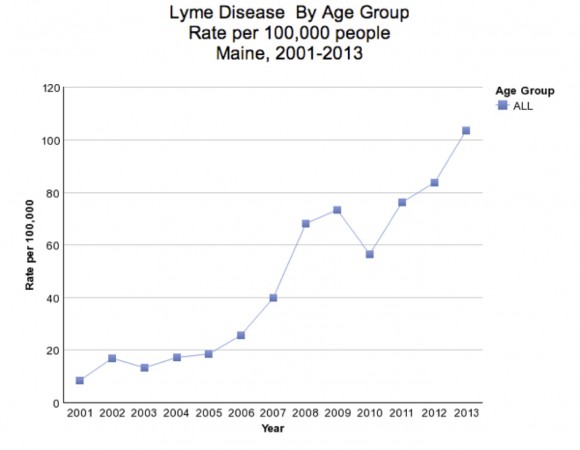
Maine.gov reference
Lyme Disease is a bacteria based disease which affects several body systems. The bacteria is transferred via the bite from an infected tick, usually (although not always) resulting in a rash in the surrounding area. The classic sign of Lyme disease is this “bull’s eye” shaped rash, although recently many cases have gone undiagnosed as people with a solid rash do not suspect Lyme Disease.
The first stage of the disease is called the Early localize stage, which begins with the rash which can take up to 30 days to appear after being bitten. Early symptoms tend to present similarly to the flu, with fatigue and joint pain being key identifiers.
The next stage, Early Dissemination begins around a week to a few months after the bite. During this stage, the disease spreads from the muscles, joints and skin into the nervous and cardiac systems. Heart problems due to Lyme disease can include blockages and weak heart muscles, thus creating symptoms such as easily induced fatigue that you would expect from poor heart function. Nervous system effects, while relatively rare, are generally serious. Common issues include meningitis and numbness or pain in certain affected nerves. If treated in or before Early Dissemination, the disease generally has no lasting effects. If the disease progresses past Early Dissemination, the patient is likely to experience lasting effects.
The Late Disease is generally many months or years after the bite. The most common symptom at this stage is arthritis of the joints, usually one or both knees.
When Lyme disease is suspected, a simple blood test can confirm Lyme Disease, although they are rarely effective within the first six weeks of the disease, and even after that can often read as a false positive. If the patient is experiencing Late Disease symptoms, they are tested for septic arthritis which presents similarly, but generally with a higher fever. A final decision on this can be achieved with an analysis of the synovial fluid, which, as we learned in BI 265, is produced by the synovial membranes, which line joints. The synovial fluid is used as a lubricant for the joint.
Treatment is relatively simple and consists of a regiment of antibiotics, which are administered via IV in more severe cases. Most patients experience lasting symptoms even after antibiotics have killed the bacteria, these patients often experience joint pain and nervous system problems for months after treatment. For patients with severe joint swelling, a synovectomy (removal of a portion of the synovium from the damaged joint) is recommended to ease some of the pain.
Fortunately, this is a very easily preventable disease. When you go outside, make sure you cover your lower extremities by wearing pants. On top of this you can also use tick repellants to deter ticks from even getting on you to begin with. At the end of any outdoor activity, make sure to check all areas of the body (especially inside joints and other warm moist places). If you ever find a tick attached to you, carefully remove it with tweezers and continue to monitor the area of the bite over the course of the next few weeks. There is no vaccine for Lyme Disease so the best way to prevent it is to be aware of the signs and symptoms and to avoid tick exposure in the first place.
Categories: Human Health
Tagged: Cal Robbins, Human Health, Lyme's Disease
February 23, 2015 · Comments Off on Calvin Robbins: The Science Behind Run Til You Puke
Have you ever heard of somebody exercising to the point of vomiting? Or have you done it yourself? I never have, but during the digestive system lecture of the BI 265 Human Anatomy and Physiology class this Jan plan I had a sudden realization as to why this happens.
While nausea may be a common feeling when working out due to food or liquids in the stomach being bounced around, that is not usually why we actually end up vomiting during hard exercise. In fact, one of the biggest causes starts with the respiratory system. The job of the respiratory system is to remove CO2 from the blood and replace it with O2. During exercise, cells produce CO2 as sugars are broken apart to make ATP, which the cell uses for energy. Some of the CO2 byproduct goes into the blood and attaches to hemoglobin, but the vast majority of CO2 is actually transported as carbonic acid, which induces respiratory acidosis. When a person is doing anaerobic activity, such as running at full speed for a long enough time, their lungs are unable to get all of this accumulating CO2 and carbonic acid out of the bloodstream thus creating increasingly acidic blood. It is not due solely to lactic acid as many people believe, but the inability to exchange enough gas in the lungs.
As the blood gets increasingly acidic, the body has to find a way to get rid of all of this acid. One of the main ways the body has of releasing acid, as you may have already guessed, is through vomiting. As you vomit, the hydrochloric acid used for digestion is expelled from the stomach, which is lined with highly vascularized rugae. As the acid is forced out of the stomach, the acidic contents of the blood are pulled out to replace the Hydrochloric acid that was lost from vomit. Following the same thought process, this is why excessive puking will produce alkalosis (high pH) in the blood.

If you vomit frequently after heavy exercise you should take a few steps to achieve a healthier and more beneficial workout:
- Base your workouts on a heart rate range. This will force you to stay within a set range for aerobic exercise, which can be roughly calculated based on your age. Usually 85% of max heart rate is the highest you should be going for an aerobic workout to prevent acidosis.
- Drink plenty of water; if you are vomiting due to dehydration, it is a much more severe issue than acidosis. Steadily drinking water before, during, and after exercise will help, as well as a small amount of sports drink to replace some of the ions lost during the work out.
It takes a lot of anaerobic exercise for the body to get to the point of vomiting. This kind of activity, contrary to what some may think, is very bad for your body, and is not something to strive for in a hard workout. Remember to drink plenty of water and keep a reasonable heart rate target in mind for a healthy and effective workout.
Categories: Human Health · Lab · Special Activities
Tagged: Cal Robbins, Human Health
February 23, 2015 · Comments Off on Rebecca Gray: Substance Abuse Isn’t F*cking Funny

I swear like a sailor around my parents. And I always have. Because my parents pick their battles, and the battle they picked was substance abuse. Substance abuse is not a joke to them. To them, impersonating the voice of a chain smoker is not funny, and the incoherent ramblings of a drunk friend are not comic storytelling material. My mother lost her brother to a drunk driver when she was thirteen, and my father lost all four of his grandparents to tobacco-related illness. Thus, they’ve always been strict with me, and the overwhelming message under their roof remains: the use of alcohol, tobacco, and other illegal, mind-altering substances is absolutely, positively, unacceptable. They spent so much time enforcing this rule and communicating its importance. Not only did I never get away with drinking in high school, I never had the inclination to; I knew how hurt my parents would be if they were ever to find out, and I couldn’t put them through that. And so, in return for 100% sobriety and transparency about where I was, who I was with, and how I was getting there, they let me swear.
I am glad this was the hill they chose to die on; I believe that I am a healthier and happier (as cheesy as that sounds) person for it. That is why Colby surprised me. The idea of drinking to the point of memory loss every weekend freaked me out. Did my friends not get that when their blood alcohol level rose too high, their brains actually couldn’t form long term memories? That when they woke up feeling like they couldn’t remember the night before, their brain in fact hadn’t truly experienced it at all? I couldn’t believe how many people my age smoked. Did they not know their skin was yellowing, wrinkling? That their lungs were turning black and their bodies becoming reliant on nicotine to function comfortably? I’ve had many a conversation with a fellow Colby student who is not familiar with the physiological effects their substance use has on their body. It is surprising and saddening to see.
Specifically, I recall a weekend last spring, during which a friend drove home with me to meet my family. That Friday, she consumed a lot of alcohol–too much– and vomited. A lot. Saturday morning, she awoke, hungover as all get out, and we trudged through the March sleet to my house. As my mom served us some soup, we chatted and caught up. It was around this time that I swore. My friend audibly gasped. “You can say that in front of your mom?” she asked.
Yeah. I can. My mom doesn’t care. What she does care about is that I don’t try a cigarette, that I don’t use marijuana without first understanding the side effects it might have on my psyche, that I don’t drink more alcohol than my liver can handle, and that I don’t rely on any mind-altering substance to feel happy. This brings me to BI 265. Having learned about the intricate system that is my body, I am even less inclined to mess around with its equilibrium. While cigarettes never tempted me before Jan Plan 2015, my newfound knowledge of arterial disease has made sure I will never get near one. I wish more parents choose to battle substance abuse with their kids, because it is so important and valuable. But even more so, I wish more people would choose to know about how their bodies work. How the things they put in their bodies, the things they do with their bodies, the things they let their bodies get near, affect their mental and physical health. Because only with this knowledge can we change substance abuse culture, both on Mayflower Hill and in general.
Categories: Human Health · Personal Story
Tagged: Colby College, Personal Story, Rebecca Gray, Substance Abuse
February 23, 2015 · Comments Off on Rebecca Gray: Healthy For All The Right Reasons
I love infomercials. I know it’s weird, but really I don’t think it’s any more shallow than tuning in to E! every week to see what the Kardashians have been up to. I remember being eight, and waking up at 5:30am to catch the Magic Bullet program on channel 8, which aired just before the Shark vacuum cleaner, which came on at 6. I’ll watch any infomercial–a brownie pan that cuts the brownies for you, a humidifier that cures asthma, a bra that somehow fits everyone. But what I’ve never been able to wrap my mind around are the fitness oriented ones: zumba work out tapes, overcomplicated pilates machines, a CD that somehow makes you lose weight if you fall asleep listening to it. I’ve thought a lot about this, and I think there are two reasons why I don’t find fitness programming engaging.
First, I’ve always felt generally okay with my body. I eat when I’m hungry and stop when I’m full. I eat leafy vegetables every day and drink mostly water. Throughout high school, I was always an athlete, and even now, I get outside pretty often, whether to ski or run or walk around a bit. In general, I’ve always been okay with my body and pretty proud of what it could do. These fitness programs prey on insecurity. People who feel okay about how they look aren’t going to spend money on a 30-day-shred work out DVD, and people who enjoy their exercise aren’t going to invest in an extravagant treadmill with separate tracks for each foot–they’re just gonna throw on their sneakers and head outside.
But second, and I think more importantly, I’ve never thought of eating or training as something I do for appearance. When I dragged myself out of bed at five in the morning to lift in high school, it was so I could shred my next ski meet. When I took up running last year, it was so I could get fast enough to train with my dad, who’s a speed demon, and spend time with him. One of the most important principles I learned in A&P is that there is more to health than looking the right way or weighing the right amount. Getting enough sleep, exercising the right amount and in the right way, eating the right things at the right times, drinking gallons of water, and limiting stress are all key. But attitude is also important. Worrying night and day about whether you’re eating the right things or running enough miles is not healthy. Obsessing over ever calorie or every hour of sleep lost is not conducive to a well-rounded life. What I’ve learned is to aim for a sustainable lifestyle of health. This includes being aware of things that are good for me (skiing and hearty, unprocessed meals) and things that are bad for me (pumpkin-chocolate chip cookies and staying up all night watching Friends on Netflix), but also being gentle with myself when things don’t go perfectly. Sometimes I’m going to have weeks where I don’t get to exercise, or nights where I stay up until 3 in the morning, contemplating the universe with friends. This is okay. It doesn’t mean I’m terribly unhealthy, and it doesn’t mean I’ve doomed my body. It means I’m human.
So yeah, I love infomercials. And I’m okay with that, even though I know TV is basically melting my brain and there are more productive, fulfilling ways to spend my time. I still find solace in the fact that I can change the channel when vapid fitness programming comes on, because I am happy with my health, both physically and mentally. I am confident that I can live well, doing the right thing for my body for the right reasons (health and fun, not aesthetic), and be gentle with myself when I am not perfect. Because let’s face it, the only perfect thing in this world is the Magic Bullet, which chops a whole onion in less than 20 seconds and is still on my Christmas list.
Categories: Human Health · Personal Story
Tagged: Human Health, Rebecca Gray
February 23, 2015 · Comments Off on Ariel Oppong: Flipped Lectures Were a Plus for Me
I am pre med and am also interested in public health especially decreasing health disparities. With these future career goals in mind taking a class such as Anatomy and Physiology could be a beneficial course choice. For the field of medicine Anatomy and Physiology is not a pre-requisite, however once a student matriculates into a medical program he or she will have to take anatomy and physiology to graduate. Thus, taking the course now could be advantageous to my schooling in the future.
A lot of past students warned me earlier that this course was very hard and time consuming, but I was still unsure if I might need it in the future so I decided to give it a chance. The first couple days were rough to say the least. We had three quizzes and a lab exam within the first week. Class was almost four hours long from 9-1pm on most days. We had lecture first and then lab for the first week and then lab first and then lecture after for the last three weeks. We were asked to sleep for 8 hours a night, to eat a balacnced diet and to try to exercise as well as complete the class at an optimal level. Prof. Klepach thought it was very much feasible but by requiring that we follow the lifestyle and do well in school what he was really encouraging was for us to find a way to study more effectively, learn better time management skills, and take our well –being seriously. For the most part I was able to exercise more regularly and eat three balanced meals but I still felt stressed and was not able to get eight hours of sleep every night.
My lack of sleep was probably at first due to the fact that we were operating on a flipped lecture style. In flipped lecture the students and I would watch youtube.com videos of pre-taped lectures and pre-taped lab lectures prior to class. Then the class would be operated with the assumption that we had done our part and had done the pre-work. During class we would complete group exercises including an overview of questions we individually came to class with. Afterwards Prof. Klepach would give us group quizzes and reviews. I found out that I really like flipped lectures. As someone that does not really learn very well by auditory means I was really happy to be provided with the pre-taped lectures because it provided me with the option to play back things that I might not have caught the first time. Moreover, the flipped lecture style allowed me to reinforce what I knew or did not know with the in class group quizzes and daily individual quizzes.
I plan to try to integrate some of the components of flipped lectures into my spring semester. I am already a junior but it seems like there are some study techniques that I have to start implementing on a daily basis. For an example I am going to try to spend more of my evenings prepping for the upcoming class instead of reviewing material that I had previously put off.
Categories: Bi265j
Tagged: Ariel Oppong, Bi265j