February 23, 2015 · Comments Off on Ariel Oppong: What is the Best Way to Study?

For Intro Into Anatomy and Physiology we had to complete both lectures and a laboratory component. For the lab part we were provided with at least an hour and a half to review the components of various models and structures displayed around the microbiology laboratory. During the first week I was excited to see the models and to see how much I remembered from the Anatomy and Physiology class I took my junior year in high school (about four years ago). The first day I realized that what I had retained from my past Anatomy and Physiology class was more broad physiology than college- level anatomy details. We had our first lab exam on day four of the class. I was shocked to find out we would have an exam so early but I do not think that it really hit me until the first Tuesday night. That night I actually came to terms with the fact that I only had one more night before the exam. Panic definitely was a feeing that immediately surfaced. I had never taken a pervious class with Prof. Klepach and I did not know how he tested so I was really worried.
Nonetheless, I had to start studying something or I was going to feel defeated before I even started. My fried Jay and I really focused our studying on the various parts of the human skull. We spent about two hours in total on that skull and we were pretty good after numerous quizzes and checks with the professor. The only issue is that by spending so much time on the skull we really did not get to study the other models as in depth. Even in the moment, I knew I was taking a risk by focusing on that body part for so long. I was just hopping that at least five or so questions would come from that region so I could reap the benefits of my studying. Haha I guess I was hopeful. My Wednesday a lot of people were over the amount of work. I think we lost about 7 people in the first week. But I was intent on finishing the class.

But was I studying appropriately? I really was not sure. In addition, I finished the previous semester pretty late, December 22nd , so when JanPlan January 5th, I was only home for around 10 days and I was pretty tired of school already. Was I putting in the appropriate amount of time? On average I was studying for at least four hours a night if you included watching the videos or podcasts for the next class, still it felt like that was the bare minimum. My first practical was really supposed to show me where my study skills were improving, okay at or lacking.

Whoa was the first lab practical hard! I did not actually study even close to the amount I needed to study in order to do well. Slacking off would be an understatement. I did poorly on the exam and the answers I got right were mainly give –away or identifications that I probably could have made even as a high school student. Disappointment was my main feeling during and after the exam. I just felt like with an exam like the lab practical- your performance is in direct correlation with your study skills. All the answers are predetermined and you just have to recognize the anatomy and regurgitate the medical terminology.

Basically my first lab practical taught me a hard lesson about slacking off plus it motivated me to try new methods and lastly it gave me a starting place that was so low that for my second exam I had no where to go but up.
Categories: Bi265j · Lab
Tagged: Ariel Oppong, Bi265j, Lab
February 23, 2015 · Comments Off on Rebecca Gray: Sociology of Epidemiology

Today, I met an epidemiologist. He spoke about disease control: how germs traverse continents, how we respond to global health crises, and how we can prepare for future epidemics, because, “after all,” he said, “they are inevitable.” To begin, he offered a bit of a crash course on HIV in America; while the subject matter was grim, the bottom line felt overwhelmingly hopeful. In a nutshell, we learned that HIV, at one time the leading cause of death for men ages 25-40 in the U.S., is now a condition well-controlled with proper medication. So yes, while HIV remains a gravely serious diagnosis, and continues to spread rapidly in underdeveloped regions of Africa, the vibe of this speech was uplifting, full of the promise of research, breakthrough, and medical revolution.
But I am skeptical. I am skeptical because this crash course glossed over the very gritty history of HIV in America. It glossed over they way AIDS (Auto-Immune Deficiency Disorder) used to be called GRID (Gay-Related Immune Deficiency). It skipped the years that HIV drugs (AZT and others) spent in gridlock, waiting to be clinically tested, because policy makers refused to fund medical initiatives for “perverts” with “homosexual tendencies”. It did not mention that the decline of HIV-related deaths in the U.S. correlated exactly with the mobilization of the gay rights movement. In short, it did not admit that disease control intersects with issues of social justice on nearly every level: race, class, gender, and sexuality.
The outbreaks we hear about, the drugs we are sold, the preventative measures we are asked to take, are carefully calculated. Information can be manipulated to reassure or scare us, to rile us up or calm us down. Our recent preoccupation with the ebola virus is a textbook example of this. As midterm elections drew near, political candidates used a health crisis occurring in Africa as ammunition in an American political debate. Articles citing the ways in which ebola can be contracted, pictures depicting its unsavory symptoms, and bold political promises to end this epidemic pervaded our lives. Then, suddenly, voting season passed, effectively closing the door on ebola discussion. This happened because government officials, now secure in their jobs, could no longer bank on public fear. In fact, our speaker did acknowledge this, and made admirable efforts to include social discussion in his lecture. It is not my intention to discredit him; I understand that in a single hour, it’s impossible to cover the field of epidemiology and all its intersections with sociology entirely. I found his presentation to be smart, well researched, and engaging. Rather, I just hope to use this blog post as a means to discuss the social implications of epidemiology in a way that we were not quite able to in class. Medicine cannot function outside the realm of social intersectionality. To say that medical information and technology are the only roadblocks, or even the largest roadblocks between ourselves and global health solutions is to be sadly mistaken. As important and exciting as medical advancement is, we must also tackle poverty and discrimination when taking on issues of global health. Class, race, gender, sexuality, age, and ableism all affect a person’s access to proper healthcare and health education.
Categories: Guest Speakers · Human Health
Tagged: Epidemiology, Guest Speaker, HIV, Human Health, Rebecca Gray
February 22, 2015 · Comments Off on Arianne Thomas: My JanPlan Experience – pt. 1

This JanPlan gave me many unique opportunities, and I learned so much about the human body in so many different ways beyond just classroom lectures. We spent hours in lab studying models, histology slides, real bones, and a real pig heart. We went on “field trips” to the art museum, where we identified different anatomical features in pieces of art, and to the athletic center, where we learned about our own heart rates, respiration, and metabolism. We completed a Grand Rounds project, which is where medical professionals present a patient’s issues and treatment for the purpose of educating medical students as well as other doctors. We were given the opportunity to work with high schoolers interested in the sciences during a mentoring session where we were taught them a little bit about what we were studying in class and helped them plan out science fair project ideas.
Some of my favorite learning experiences organized by Dr. Klepach was bringing in different speakers who talked to us about what they do in their day to day lives and the issues they seek to fix. The first speaker was Dr. Zak Nashed, a radiologist who specializes in peripheral artery disease. PAD is a circulation problem where arteries that supply blood to the extremities get clogged by the hardening of arteries, often times leading to a stroke or a heart attack. It can cause damage to the endothelial lining of the arteries, an increased permeability and adhesion of molecules, and if it goes untreated there could be a complete obstruction. One treatment option is medical management, where the risk factors could be modified (by exercising, losing weight, or stopping smoking) or a pharmacologic intervention could be used to regulate hypercholesterolemia, hypertension, or diabetes. Another treatment option, which Dr. Nashed specializes in, is interventional radiology through endovascular techniques. These are minimally invasive procedures where medical professionals use image guided tools to perform balloon angioplasty and place stents to open up narrowed arteries due to plaque build up. The third and most extreme treatment option is to perform a bypass graft or an amputation.
The other speaker who came to talk to us was Dr. Peter Millard who is an epidemiologist, someone who studies causes and patterns of diseases in different populations. He talked to us about his work with diseases in Africa, making the interesting point that where he worked in Mozambique is about the same distance from Liberia as it is from New York, but in reality New York is a lot closer because there is more traffic between the two places. He explained that geographic proximity is different from travel patterns and the way disease spreads has a lot more to do with traffic than geographic proximity. He also talked about the prevalence of HIV across different parts of Africa, and possible correlation between these rates of HIV and circumcision. Another interesting aspect of epidemiology he talked about was the importance of disease prevention on economic and social levels.
Having these speakers come in to talk with us was an integral part of my learning experience in the Anatomy and Physiology class because it opened my eyes to all the various aspects that the sciences, biology in particular, encompass. Having both parents working in the medical field has always fostered an interest in a profession in the medical field, but I have never had a concrete idea of what I specifically would like to do. These opportunities of having two very different speakers come talk to us made me more aware of the various directions my degree in biology can take me and interested in looking into different careers that I would have never thought about before.

Categories: Bi265j · Guest Speakers
Tagged: Ari Thomas, Bi265j, Peter Millard, Zak Nashed
February 22, 2015 · Comments Off on Arianne Thomas: My JanPlan Experience – pt. 2
Going into my first JanPlan two years ago I didn’t know what to expect. The only thing I had known about it that it was a time to step out of your comfort zone, take a different class, and explore other aspects of learning. I signed up for the Catholic Church and Hollywood class that year because it fulfilled two distribution requirements. I thought that the class would be a breeze. Not only did I hear from upperclassmen that it was an easy class, I was also raised in the Catholic Church and went to a Catholic school for most my life, and therefore had to take church history and other religious classes throughout my high school experience. Turns out, the class was easy. The class met three times a week, and every single day we watched a movie, the hardest part of the class being keeping my eyes open for three hours in the dark room. There were three relatively short essay assignments and there was no final.
My sophomore year, I decided to step out of my comfort zone. I took the African Music class being not at all musically inclined other than my experience with the recorder in the third grade. Since the class fulfilled the art distribution requirement, and I’m even less artistically inclined, I figured I would manage. A normal class day consisted of singing, drumming, and dancing. There were no assessments other than a few performances at a local church and during the Martin Luther King Day celebration.
I knew this year would be different when I signed up for Anatomy and Physiology. My mom, a retired flight nurse in the Air Force, recalled taking full semesters of both Anatomy and Physiology while in college. She was surprised that we could fit in all the information in just one month, recalling specific parts and functions of the human body that she was required to know. I knew it would be a lot of hard work, but I was prepared to dedicate my month to working hard. Going over the syllabus on the first day, I was a little bit overwhelmed with the amount of material, quizzes, and projects we were going to accomplish during the month. Dr. Klepach also warned us that people often get C’s and D’s on the quizzes and tests, which was worrisome as my grades and my GPA are always a primary concern. On top of it all, our professor wanted us to keep logs of our eating, exercising, and sleeping habits and to monitor our stress levels. Within the first few days of the class, I was completely overwhelmed by all the work and studying I had to do and called my mom for some support, only to hear her say “I told you so.” It was a matter of days until about a third of the class switched into a different class. The first week proved to be the hardest, listening to two hour long lectures and taking detailed notes on top of studying for a few quizzes and a lab test. It was really encouraging to hear Dr. K’s words of praise after the class average on our first lab test was 40%, well above the average of last year’s class. Although the subsequent weeks lightened up and my personal scores improved, the most important lesson I learned was balancing my life. Previously, when I got swamped with school work, I would often cut out exercising or a full night’s sleep to catch up with work. Dr. K stressed the importance of a healthy lifestyle, and this transformed me to be a better student. It not only forced me to stay on top of my work, but also kept me healthy during the time of the year when many people get sick. This aspect of the class was crucial in showing me that a healthy, balanced lifestyle can be achievable even with a rigorous school schedule, which is something I believe many college students tend to forget.

Categories: Bi265j · Human Health
Tagged: Ari Thomas, Bi265j
February 22, 2015 · Comments Off on Lauren Shirley: Cardiology: Getting to the heart of the matter

One of the highlights of my experience in BI265j was the cardiac section and in particular, the heart dissections we got to do. I had a fairly solid understanding of the heart coming into the class from my EMT training. I knew that the blood came into the heart through the vena cava entered the right atrium passed through the tricuspid valve to the right ventricle, was pumped to the lungs through the pulmonary arteries to receive oxygen and then returned to the heart through the pulmonary veins into the left atrium then through the mitral valve to the left ventricle and out to the ret of the body through the aorta. What my EMT training had failed to teach me, however, was the beauty of this process, which is almost artful in its simplicity and elegance. This class gave me a greater appreciation of the elegance of the heart and the mechanisms behind its continuous beating. I was fascinated by the spread of electrical signal and its motion through the myocardium. The depolarization starting at the sinoatrial node, which spreads to the atrioventricular node then through the bundle of His and out to the Purkinje fibers is a highly linear path, simple yet powerful. While the lecture on the heart and studying plastic models in lab fascinated me, it was the opportunity to dissect the heart that truly solidified by understanding of it.

We dissected preserved cow hearts. Initially, I was impressed by the thickness of the muscle in the heart walls. It took quite a bit of work with a scalpel and scissors in order to get down into the different chambers of the heart. The sheer thickness of the walls and the work it took to get through them spoke to the sheer power of the heart as a muscle and the strength needed to supply a large body, such as a cow, with blood. Once inside the heart, I was fascinated by the sheer strength of the chordae tendinae, the fibers that keep backflow from occurring in the tricuspid and mitral valves. Despite pulling on these relatively thin cords, they didn’t tear! This further illustrated the necessary strength of the heart to me and the great pressure and quantity of blood that it pumps.

While it was really exciting to get to see a real life illustration of the models we had studies (that wasn’t color coded), it was even better to have a chance to share our newfound knowledge of the heart with the high school students who visited. I felt that teaching them what I knew solidified it in my mind. However, it was also exciting to see the “next generation” of young science students and how fascinated they were with the human body and its functions. I felt that my enthusiasm for cardiac function was almost contagious as I eagerly showed them how to dissect ad encouraged them to explore and understand the heart in front of them.




Long story short, this class got me pumped for cardiac anatomy and physiology and a possible career in cardiology. Ironically, I love the heart!
Categories: Bi265j · Lab · Special Activities
Tagged: Dissection, High School, Lauren Shirley
February 22, 2015 · Comments Off on Allison O’Connor: Heart Dissection

Although I took a lot of science classes in high school, I never had the opportunity to do any dissections. Dissections were always something wanted to get to do because I feel like the best way to learn is through hands on experience. I first fell in love with anatomy in middle school when I visited the Body Worlds exhibit while it was in Philadelphia. My dad took me to this exhibit expecting that we would walk through quickly, but instead we were there for hours as I stopped and closely examined every part of the exhibit. This exhibit was the closest I ever got to dissecting anything before this JanPlan, but the exhibit definitely inspired me to want to learn more about anatomy.
In my various science classes and in my emergency medical technician training I had learned about the basic structure and function of the heart. Numerous times I have been asked to trace a drop of blood through the heart and it is something that I could recite in my sleep. When we started the cardiovascular unit in anatomy and physiology this JanPlan I thought I was going to hear the same spiel about the heart that I had heard so many times before. However, this JanPlan, I saw the heart in a whole new light. Though I had already learned the basic function before I learned about the anatomy in much more detail this month than I had in the past. I also learned more about the electric conductance system of the heart and some very basically how this presents itself on an EKG, which is particularly interesting to me since I see EKGs done by the paramedics on the ambulance all the time.

The heart and its function have always been interesting to me, however, I did not fully understand how truly amazing the heart and its structure are until I was holding the pig heart in my hands. While the heart was in my hands I was able to identify the structures that I have learned about so many times and really see for myself the relationship between the structure of the heart and its function. Being able to literally stick my fingers through the arteries and veins to feel where they went lead me to understand the structure of the heart on a whole other level. I was amazed at how muscular the walls of the heart actually are. You are always told that the heart is an incredibly strong muscle, and it is a fact that you just blindly accept as true, but holding the heart in my hands and trying to cut through the muscular walls really showed me the true strength of the heart muscle. I was also surprised at how strong the chordae tendonae were given the fact that they look no stronger than a strand of floss. I put their strength to the test by pulling on them with lots of force and was unable to break them. The heart dissection reminded me of the importance of hands on learning and learning through discovery as opposed to just blindly accepting things as fact. When you blindly accept things it is easy to lose sight of the intricacies and wonder involved in the systems around us. I was in awe during the entire heart dissection and it really changed the way I thought about the cardiovascular system and reminded me of the importance of being curious and full of wonder.

Categories: Bi265j · Lab
Tagged: Allison O’Connor, Dissection, Lab
February 22, 2015 · Comments Off on Allison O’Connor: Grand Rounds Presentations
As a part of our Anatomy and Physiology course this Jan Plan, we worked in small groups to research and present a case study to our peers and a few health care professionals during a mock Grand Rounds presentation. Grand Rounds is a tradition in the medical field in which physicians present case studies to their peers, other medical professionals and medical students on a medical topic to share things that they learned in particular cases, so that others can learn from these cases. The Grand Rounds presentations were a highlight for me this JanPlan. Not only was it interesting to explore a case study of our choosing and get to learn about a particular medical condition, but it also exposed me to the format of Grand Rounds presentation and gave me the opportunity to practice my public speaking skills (which is something that is very anxiety provoking for me).
My group used the New England Journal of Medicine’s database to find a case study that we all found interesting. After reading through various case studies, we settled on the case of a 32 year old female, who three weeks post partum presented to the emergency department with substernal chest pain that radiated to her jaw. Substernal chest pain can be a result of many different complications including: cardiovascular complications, respiratory problems, gastrointestinal complications and musculoskeletal problems. Although cardiovascular complications are the most common cause of chest pain, it is not typically a complication that is expected in an otherwise healthy 32-year-old female. However, the fact that this patient was postpartum increases the index of suspicion for myocardial infarction, pulmonary embolism and coronary artery dissection because of the hormones present during pregnancy. An angiogram in the emergency department revealed a left anterior descending coronary artery dissection with a 35mm segment of narrowing and 90% stenosis.
Coronary artery dissections occur when the inner and outer layer of the coronary artery separate and blood pools in the area between the layers, causing decreased blood flow to the heart. There are two major types of coronary artery dissections, those that are spontaneous and those that are mechanically precipitated. Given this patient’s postpartum status and the events that precipitated her dissection, her coronary artery dissection would be classified as spontaneous. Within spontaneous coronary artery dissections, there are four sub-classifications, however only two of those are relevant to this case: postpartum coronary artery dissections and idiopathic spontaneous coronary artery dissections, which are dissections that are result of increased hemodynamic pressure caused by shear stress. Based upon test results, the patient’s postpartum status and the lack of disease in her other arteries, the patient was diagnosed with a spontaneous postpartum coronary artery dissection. Since postpartum spontaneous coronary artery dissections are relatively rare, there is not a universal treatment protocol. Conservative treatment is preferred, however sometime more invasive measures are required. In this case, conservative treatment was the most appropriate plan since the patient was stable, was experiencing very little pain and only had slight cardiac ischemia. The patient was treated with an intra-aortic balloon pump for two days to make her coronary artery more patent and was also given β-blockers, aspirin (an antiplatelet agent) and heparin (an anticoagulation agent). After two days, the patient was showing significant signs of improvement and was discharged from the hospital after eight days. The patient was able to return to life as normal and at the time that the case was presented had no further complications.
Since we had used the New England Journal of Medicine database to find our case study, we were actually able to get our hands on the PowerPoint that was used in the original Grand Rounds presentation given at Massachusetts General Hospital. The PowerPoint contained videos from the angiograms done in the hospital as well as other helpful pictures and background details of the case that we would not have had access to if we had not been able to obtain this PowerPoint. Having the actual angiogram videos from this patient enhanced our presentation immensely and made the case study feel more real.
I found this topic to be especially intriguing because it combined two of my clinical interests: women’s health and cardiology. I have always been drawn to women’s health issues particularly pregnancy and birth and for a while now have considered becoming an OBGYN or midwife. Spontaneous coronary artery dissections (SCAD) are a rare complication of pregnancy, so it was really valuable to learn about the presentation and treatment options for SCAD and this knowledge could potentially be useful in my future career, which made the information feel very relevant. This JanPlan I discovered a new interest in the heart and cardiology. I had never considered cardiology to be a field I was particularly interested in, but the cardiovascular unit in this class really opened my eyes to the wonders and intricacies of the heart and has left me wanting to learn more. This topic fit my interests perfectly and I thought it was really cool that we got the opportunity to study a case and explore our personal interests in an incredibly relevant way. Postpartum SCADs are very rare and are often overlooked, but now I know what to look out for which will hopefully help me provide the best care possible to my future patients. I also felt that I learned a lot of important and relevant information from my peers presentations. It was really fun to get to watch my classmates present topics that they were passionate about. Grand Rounds was a very rewarding and interesting endeavor and was definitely a highlight of my month.
https://www.youtube.com/watch?feature=player_embedded&v=bODWv-x-eDc
Categories: Bi265j · Grand Rounds
Tagged: Allison O’Connor, Grand Rounds
February 22, 2015 · Comments Off on Alexandria Lucas: Grand Rounds / Oligoastrocytoma

The grand rounds project, which consists of research on a particular topic and a final group presentation that is open to the public, I think was perhaps one of the most valuable parts of this class, for it really did require a lot of individual learning and the students really had to take things into their own hands, be independent, and put a final product together all outside of class, much like the way things will happen in medical school. I very much appreciate that Dr. K always pushed us to work hard in this way to prepare us for much harder tasks that are to come in the future in our post-Colby years, and the Grand Rounds project was easily one of those things.
My group wanted to do a case study for our project, so we first began by looking through a list of different case study articles when one caught our attention titled: “32 year old woman with episodes of unconsciousness.” We were very curious what was causing these episodes, because it really could be a wide range of things, so we choose this as our topic because of its very intriguing symptoms.
The next part of the project consisted of breaking up the material into sections, such as symptoms, differential diagnosis, diagnostics tests, and more, and then each group member doing research on their assigned sections. We then worked on putting together a PowerPoint presentation and a one-page synopsis on the topic. Some groups did a lot of this work together, but it is always hard to find a time that everyone can meet, so we ended up doing most of this work alone and communicating over email and Google docs which I think actually worked really well.
On the second to last day of class, each group presented their PowerPoint on their topic for about 15 minutes. I found this to be one of my favorite class times throughout the whole semester. I really enjoyed hearing about medical cases that I know nothing about, as well as see the different groups be so intrigued and excited about the topic they choose to research, and in addition seeing how much knowledge we had all gained over the past few weeks.
It was, however, a little nerve-racking to be put in front of the class speaking about something that is often quite advanced and perhaps a little over a college students’ head, but having the class there and Dr. K in front being very supportive, the presentation did not end up being as scary as I thought it was going to be. Our case, of the 32 year old woman with episodes of unconsciousness, was mainly a result of an Oligoastrocytoma, which is a tumor consisting of mixed cells. It was located in the temporal part of her brain, which was causing her unconscious episodes. However, what makes this case even more interesting is that she had a genetic predisposition to neurocardiogenic syncope (fainting, loss of muscle both due to abnormal control of the brain over the heart), which led to her case being complicated by ictal asystole (stopping of the heart during her epileptic seizures, which is very rare). Not only during this Grand Rounds project did I have the opportunity to be an independent learner as well as a group member, but I also learned a significant amount about this woman’s case and Oligoastrocytoma’s, as well as recognizing the fact that although certain medical cases can easily explained by one disease, that does not mean that is always the only thing going on.
https://www.youtube.com/watch?feature=player_embedded&v=bODWv-x-eDc
Categories: Bi265j · Grand Rounds · Human Health
Tagged: Alex Lucas, Grand Rounds, Oligoastrocytoma
February 22, 2015 · Comments Off on Alexandria Lucas: Overall Experience
Coming into this class, I had heard it was going to be a lot of work and was certainly not going to be a walk in the park. With that said, I had significant interest in Anatomy and Physiology, mostly because I have never had the chance to take a class on this subject material. Thus, going into it I know I was driven to work hard and I would enjoy putting effort into it to take on the challenge of learning so much anatomy and physiology in the four-week period. I have to say the first week of this class was certainly the hardest of all the four weeks, and definitely scared me a little. Yet, I know that in that first week I probably had my time of greatest learning as far as how to study the material most efficiently while still maintaining healthy life habits, which is one of the main goals of Dr. Klepach’s in this class. With 3 quizzes that week and a lab exam on tissue, bones, and muscles, it was nowhere near an easy first week. However, making it through that first week was incredibly rewarding.

In addition, during that first week of class we actually ended up trying a flipped lecture. This meant we would watch recorded lectures from last year and then go into class and do review, answer practice questions, and activities for engraining the material in our head and helping us to understand it better. I had never done a class like this before, so it was very interesting to experience. However, the next week the class vetoed to have normal lectures.

Overall, I think that the lab tests were definitely the most stressful part of this class. For the first one, I truly believe I did not understand the amount of time you had to put into studying the anatomy nor had I yet realized what studying method was going to work best for me. For that first lab exam, I really only looked over the PowerPoints for a decent amount of time. I soon learned that was not going to cut it for studying for the exams, in which you walk around the room and identify not just major muscles on the models, but rather the small muscle that goes around the top of your eye or the specific name of a vertebra, for example. It is not meant to be easy. Needless to say, that first lab exam did not go very well for me at all. However, for the second exam I realized it may help to interact with the models, since after all, that’s exactly what we were going to have to recognize anatomical features on for the exam. Although I still did not do incredibly well on the exam, I made a clear improvement in my grade from the first exam, which was definitely an accomplishment as well as what Dr. K hopes students to do during his Janplan class; find what studying tactics work best for your and improve over the course of the month.

Categories: Bi265j
Tagged: Alex Lucas, Bi265j
February 22, 2015 · Comments Off on Rachel Bird: Heart Dissection

I know, rationally, that the brightly colored red and blue heart diagrams in the spiral bound textbook on the lab table aren’t entirely accurate. However, I was surprised at how disappointed I was to open the box of shrink-wrapped pig hearts and discover that the entire heart is a homogenous beige color – somewhere in between tea with too much milk in it and the thick clay in the riverbeds near my house. Luckily, that disappointment didn’t last. As my lab partner, Rebecca, and I unsealed the plastic wrap, our first impression of the heart was the smell. Acidic, chemically, headache-inducing: the preservatives that kept our heart from smelling like rotting meat also made the entire lab smell like the inside of a formaldehyde bottle!


As our noses adjusted, we began our cursory inspection of the heart. Once I was able to get over the bland coloration, our pig heart actually looked remarkably like the textbook model. From the shriveled atria to the rubbery arteries, our pig heart just looked like a small-scale reproduction of the plastic hearts that had been on display on the lab tables all week. Once we oriented the heart with the apex pointing down, Rebecca made the first cut, deftly slicing the heart in half like a bagel. We both gasped. The interior of the large, muscular ventricles was covered in delicate, stringy chordae tendineae! The textbook photos and models mentioned these fibrous bands, but the lightly sketched lines in our reference image in no way prepared us for the network of elastic filaments that criss-crossed through the ventricles. Rebecca tugged at one of the strands, but instead of breaking, it snapped back into place as soon as she released it. Those things are a lot stronger than they look!
Our second surprise was the septum’s thickness. We had both memorized the fact that the left ventricle has stronger muscle walls than the right ventricle (because while the right ventricle only pumps blood back into the lungs to get oxygenated, the left ventricle has to distribute blood to the entire body). However, the difference was huge! The septum was thick and muscular and not at all thin like the cartilaginous septum that separates the nostrils. As we continued to hack away… or rather, “dissect,” our heart, we noticed that if you pulled the filmy visceral pericardium away from the outer walls of the heart, it revealed rougher, almost striated muscle tissue below. It was even possible to pull up small strands of muscle tissue with the tweezers and separate the layers of the heart muscle. The same was true of the interior of the ventricles – once we peeled back the smooth endothelium that protected the inner walls of the heart, the coarser muscle tissue was revealed.
Even more interesting than the layers of the heart muscle was the layered structure of the veins and arteries splaying out of the heart. After Rebecca and I had thoroughly examined all the entrances and exits to the heart (mostly by sticking our fingers in the tubes to figure out which chamber each one led to), we sliced off a section of the aorta and attempted to identify the layers of the tissue that compose an artery.
By the time we were finished, our pig heart lay in chunks all over the dissecting tray. Rebecca was poking one end of her tweezers through the coronary artery and I was still stubbornly trying to “de-fat” the right atrium. As class time ran out, we reluctantly cleaned up our heart and threw out our gloves, eager to get the scent of preservatives off our hands. As Rebecca and I threw out the last of our paper towels, I turned to her and said, “I hope they aren’t serving pork carnitas again at lunch. I don’t really think I can imagine eating pork after that…”
Categories: Lab
Tagged: Dissection, Lab, Rachel Bird
February 22, 2015 · Comments Off on Mayra Arroyo: The Heart Dissection

The activity I enjoyed the most during this class was the pig’s heart dissection. As a student, I, sometimes forget that the diagrams and figures in textbooks are only a close resemblance to what things actually look like. This is especially true when dealing with the human body. Diagrams are usually different colors and are embellished to in order for students to learn them more easily. At first it was a challenge to find the parts of the heart I had only previously learned via diagrams. There were many times I could not find the correct anatomy for examples the pulmonary vein and the aorta looked very similar on the real heart, so it was hard to distinguish between them. Another thing I did not realize is the strength and thickness of the heart’s wall. At the start of the dissection I was extremely cautious of how deep I cut into, but I started to realize that the heart was very thick and strong. This activity showed me that the heart is truly amazing part of the body, which the diagrams did not do justice.


One of my big triumphs during this activity was locating the coronary arteries on the pig heart. Although by just looking at the outside of the heart it is possible to see where they are, but we were able to see where they connected to the aorta and where they extend away. We were able to stick a probe and follow them. We removed some of the fatty tissue to see a clearer view of the arteries. It was amazing to see these arteries, because at that point I knew my presentation was going to be about coronary artery disease and its possible treatments.


Dr. Klepach told that class that you do not really know and understand material until you teach it to another person. I had the great pleasure to put this idea to the test with the heart dissection. We showed high school students how to dissect the pig’s heart. This was a great learning experience for me, because I was able to solidify the anatomy I already knew, and it also taught me what I had missed the first time. This was by far the most useful part of this activity for me, and the most valuable. I became a full believer in this idea, and will continue to use this strategy in my future studies.
Before this unit I knew only very basic concepts of the heart’s function and its anatomy, but after this activity and lecture my knowledge increased greatly. I am biology major with a concentration of neurobiology and I thought I wanted to go into the neuroscience field, but after this unit I am seriously considering going into the field of cardiology. This is a very challenging topic, but it can potentially be a very rewarding subject for me. There is still a lot I do not know about the cardiovascular system, but I am eager to learn much more about the heart and it’s importance to the human body.

Categories: Bi265j · Lab
Tagged: Dissection, Lab, Mayra Arroyo
February 22, 2015 · Comments Off on Yvette Qu: My Overall Experience This Semester

Taking Human Physiology and anatomy as a freshman, I have found the course to be appropriately challenging and a great introduction into biology major. In the first few days of the course, the materials were somehow overwhelming to me. Everything needed to be memorized, and preview and review are required to do well on the quiz. However, the stress level was what I was expecting. I was hoping to learn more about biology and to decide if I can major in biology. Therefore, though I was a little terrified at first, I continued to work hard in the course, and I did gain more than I expected. Dr. Klepach had quiz after almost each lecture, and this stressed me out at first because I did not have the habit of reviewing things after each class. Being a procrastinator, I was more prone to leave everything before the finals despite the fact that I knew it was a bad habit. This course helped to reform my study methods. I have developed the habit of previewing and reviewing for each class, and the new method works perfectly. Another issue, which remained to be challenging, was the huge amount of terms of the labs. It was extremely difficult to remember hundreds of terms of minor body parts and to avoid forgetting them before the lab tests. For many time during the tests, I knew I had memorized the name of the model but could not remember how to spell it or the complete name. I did poorly on the first lab tests, but I had to admit that I did not work hard on the labs as I did for the lectures because I procrastinated the memorizing task to the last night. Despite the laziness, I forced myself to review for each lab, and as a result I did improve a lot from the first lab test to the second one. I am sure the reason is the amount of effort I put in for the second lab test. By the end of Jan Plan, I have been much more familiarized with human body than I was. The mysterious and complex human body amazed me so much that I cannot wait to learn more. My goal of learning more about biology and deciding if I want to major it was achieved, I have found myself interested in biology. Overall, I enjoyed the course of Human Physiology and Anatomy a lot and gained more than I have expected. Most significantly, this experience solidifies my decision of majoring in biology. Moreover, I have developed a better study method. Avoiding procrastination and just simply finishing preview and review for each lesson, I arrived at the score I am satisfied with, and I believe this method will help me to do better in any future courses. One more thing, with the time sheet, I did lead a healthier lifestyle in January, sleeping enough and eating regularly, than I did last semester. I would absolutely recommend this course to anyone interested in biology and ready to be appropriately challenged.

A specific activity that I particularly enjoyed:
I had a mixed feeling toward the quiz after each lecture. I really hated them at first because they forced me to study after each lecture and challenged my bad habit of procrastination. Also, I was panic when Dr. Klepach said that the average grade for the quiz was a C or D for the past years. In order to get a score higher than a C, I reviewed with extreme attention everyday. At first, it was very difficult to fight against my laziness and painful to avoid procrastination. I was frustrated when my friends taking easy Jan Plan courses had nothing to do while I had tons of things to review. However, my efforts did pay off. I did pretty well on the quiz and I was very satisfied. I begin to enjoy the result coming with the painful procedure of fighting against procrastination. Though I did know working hard and stay on top of everything could bring much better result than procrastination and laziness do, but knowing something and actually experiencing something was very different. Knowing working hard would help did not motivate me to actually do so, while when the quiz forced me to work hard and I did experience the result of the effort, I was motivated. My feeling toward the quiz changed from hatred to enjoyment and thankfulness. After well preparation, the quiz became a great ways to examine my mastery of knowledge instead of a frustrating torture. Moreover, the quiz helped to reform my study method to a better one. Even though the beginning of the forcing from the quiz was painful, the change it brings will benefit me in an unpredictable way in the future. The habit of previewing and reviewing can make me understand and memorize things better through the repetition of content from each lesson, which is much lesser amount of things than whole semester. Another thing to mention, this daily study habit not only brings better grade, it also improves efficiency and helps me to lead a healthier lifestyle. By procrastination, I left a huge amount of work to do the few days before exams; while I stayed late in those days before exam, I just wasted time irrationally on other days. Staying up late means low efficiency and unhealthy lifestyle. However, with the newly formed study habits, previewing and reviewing for each lesson, I put a reasonable amount of work for each day; the reasonable amount of work can be done without staying up late, and thus efficiently. The quiz offered was a boon, for the change it brought to me will benefit me in any courses in the future. Knowing how procrastinated I was, I did not anticipate the course to change my study habits so radically, but it does and I really enjoyed the change. Just as Dr. Klepach said, the course not only helps the students to learn biological knowledge, it also helps the students to from a better and healthier learning method and even lifestyle.


Categories: Bi265j
Tagged: Bi265j, Yvette Qu
January 31, 2015 · Comments Off on Danielle Levine: My Experience in Bi265j
Danielle Levine (’15, Biology)

To complete the Biology major at Colby, one has to take a minimum of six biology lab classes. As a senior biology major who at the end of the fall semester needed to take one more biology lab class, I chose to sign up for BI265 Introduction to Anatomy and Physiology for my January course rather than take an additional lab course (I will be taking the second semester of physics, which also has a lab) in the spring with my busy tennis team schedule. Having been warned before the class started that anatomy and physiology courses are a lot of work and a whole lot of memorization, I was expecting and prepared for an intensive month – but as the first week started, I found I was not quite ready for this class! During the first week, I was very nervous about the class – very concerned and stressed about the workload – and I remember wondering if I made the right decision to take the class, or if I should have just taken another lab course in the spring. After having now finished the class, I am very grateful for the opportunity to have taken BI265 with Dr. Klepach, as I truly enjoyed the class (excepting, of course, that first very difficult week!) to the fullest extent. I would recommend this class to every biology major, pre-med student, or any student at Colby just interested in learning how the human body works.
The class was, in fact, a lot of work, from studying for quizzes for almost every lecture, to listening to podcasts of lectures and labs for the next day, to making and presenting a Grand Rounds powerpoint to physicians and nurse practitioners, to studying for hours on end memorizing and identifying different anatomical structures and features on plastic models in the lab. However, the amount of material I learned and the understanding I achieved with respect to the structure and function of the human body was unimaginable to me before I took the class. The sheer volume of knowledge to be gained from this course is reason enough to recommend this class to other Colby students.
As a pre-med student, I am easily caught up with concern over my grades, GPA, exams and assignments, but taking this class reminded me of the importance of seeking to understand and learn material for oneself and for one’s own knowledge rather than for the primary purpose of getting a certain grade on an exam. As I hope to become a medical professional one day, this class had many practical aspects beyond the classroom; I was able to practice presentation skills via the class’s Grand Rounds presentation project, build a foundation of human anatomy and physiology for medical school (which I hope to go to!), learn how to succeed under stressful situations, and finally, balance my schedule keeping in mind the importance of maintaining a healthy lifestyle.
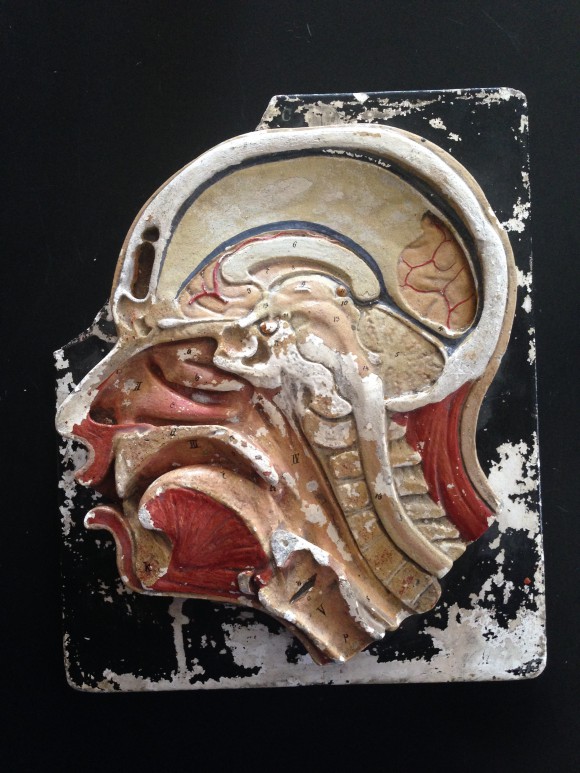
In taking this course, I was given many wonderful opportunities, such as being able to perform a wet dissection of a pig heart, and then being able to help visiting high school students perform a dissection on another pig heart, teaching them and sharing with them the material I had learned about the cardiovascular system the week prior, listening to guest lecturers, including Dr. Zak Nashed, who discussed interventional radiology and peripheral artery disease, and Dr. Peter Millard, who spoke about the field of epidemiology. Overall, I enjoyed this course very much, as it was a wonderful opportunity that I believe prepared me for the future after I graduate from Colby this spring, and reinforced my decision to pursue a career in medicine.



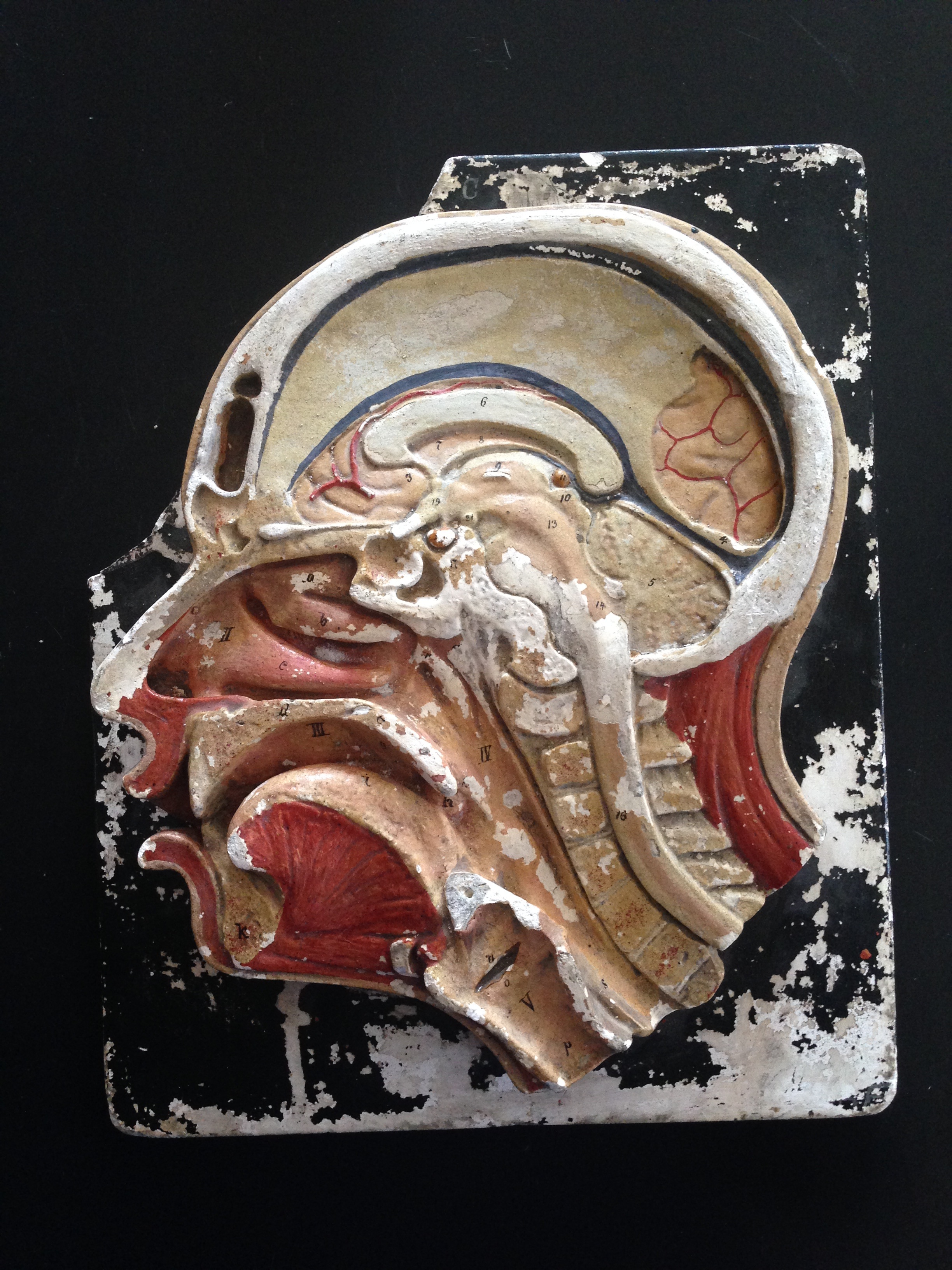
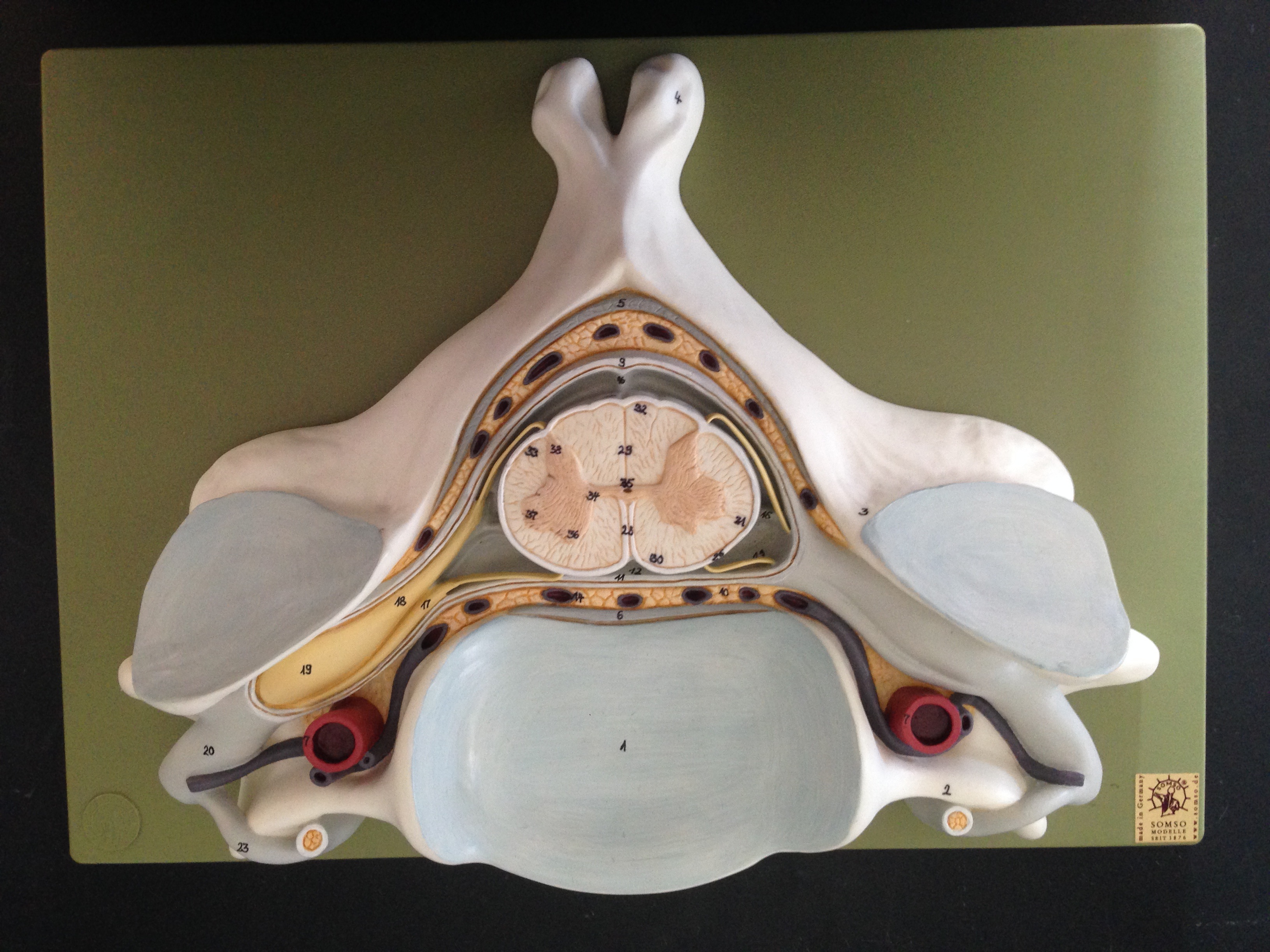
Here are some of the models used during lab and for studying for the lab practical exams.
Categories: Bi265j
Tagged: Bi265j, Danielle Levine
January 31, 2015 · Comments Off on Danielle Levine: Grand Rounds
Danielle Levine (’15, Biology)
One of the opportunities I had during this Jan Plan course was to participate in a Grand Rounds Presentation; Grand Rounds, in which physicians give lectures to their peers, including other physicians and medical students, on a medical topic is a common tradition in medical education. In groups of three students, we were able to pick any topic of interest for a fifteen minute oral presentation that we would present at the end of the semester. Given the vast array of medical topics that could be picked for a presentation, we looked to academic medical sources, including the New England Journal of Medicine, for possible past case studies that we could research and discuss. After scrolling through dozens of case studies, and clicking on articles with titles that seemed very interesting and then reading the articles’ summaries, we finally settled on an interesting case subject, one about celiac disease or gluten-induced enteropathy, that we considered particularly relevant given the current emphasis on the effects of gluten in the diet in popular culture.
In this case study, a 42-year old man presented to the emergency room with the chief complaint of chest and abdominal discomfort; given his additional history of unintentional weight loss and chronic diarrhea for ten years following coronary artery bypass grafting, an inflammatory disorder or a cancer of the chest or abdomen were differential diagnostic considerations. After multiple tests were performed, including an invasive exploratory laparotomy done after a CT scan showed enlarged jejunal lymph nodes, a small bowel biopsy revealed the diagnosis of celiac disease given the presence of flattened villi and intraepithelial lymphocytes. Today, celiac disease can be diagnosed via a simple blood test for IgA tissue transglutaminase and IgA endomysial antibodies. This case study demonstrates the importance for physicians, especially given the increasing incidence of celiac disease, to test for it non-invasively when a patient’s symptoms may be suggestive of it.
The diagnosis of celiac disease has been increasing in the developed world, at least in part due to the availability of new non-invasive tests to diagnose the autoimmune disorder. Also, there has been an increase in the diagnosis of non-celiac gluten sensitivity, which has been an even more significant factor in the increase in the number of people now adhering to a gluten free diet in the developed world. Unfortunately, some people do not have a true gluten-related disease or sensitivity, but are adopting a gluten free diet in a fad-like way. This is unfortunate because a gluten free diet can cause its own problems, such as nutritional (in particular, certain vitamins) deficiencies, and a lack of fiber in the diet leading to bowel-related issues.
Given the occurrence of a generalized increase in autoimmune disorders today, the hygiene hypothesis has been offered as a possible explanation, the basic tenet of which is that given increasingly prevalent strict hygienic practices, children today are exposed to fewer pathogens, and as a result can develop autoimmune disorders in which their own immune systems attack self antigens. Given the increasing numbers of people diagnosed with autoimmune disorders, it is hoped that research into celiac disease as well as other autoimmune disorders will lead to improved treatments of and ways to prevent them.
This Grand Rounds presentation was very informational as it allowed us to research a current topic of interest and, in so doing, learn the signs and symptoms that may exist at presentation of a certain disease (in this case, celiac disease), and how that disease may ultimately be diagnosed. As celiac disease is likely to continue to be a relatively common disease in the developed world, I believe this experience will be helpful to me, since I hope to become a physician someday. Being able to present our research to our peers as well as physicians and nurse practitioners, that is, to emulate something a real physician might engage in, was a wonderful experience. Furthermore, my mom, as a physician, talks about attending Grand Rounds Presentations every week at a hospital in New Jersey, and for me to be able to present a case study in the same manner was a fun and great opportunity.
http://youtu.be/DiKDOyG6Olg
Categories: Grand Rounds · Human Health
Tagged: Celiac Disease, Danielle Levine
January 31, 2015 · Comments Off on Cameron Matticks: JanPlan 2015 Internship talk to Bi265j Human A&P
Cameron Matticks, (’15, Cell & Molecular Biology) was the 2015 Bi265j TA and intern. Listen to his talk to the class about his experience below.
http://youtu.be/1uU5Tpgoaf8
Categories: Guest Speakers · Human Health · Internship Talks
Tagged: Cameron A. Matticks, Internship
January 30, 2015 · Comments Off on Dr. Peter Millard, Epidemiologists Comes to Speak.
The last day of class we had the pleasure and honor of hosting epidemiologist Dr. Peter Millard, an MD PhD based in Belfast Maine, for a thoroughly engaging hour as he spoke about a wide range of epidemiological issues. The topics covered spanned his work on HIV infection in Africa, to the political, media and social components of disease right here in Maine.


For all of the students in Bi265j I would like to thank Dr. Millard for graciously donating his time to come and speak to us. Watch his interesting and informative presentation below.
http://youtu.be/RFzfVgixaZU
Categories: Guest Speakers
Tagged: Epidemiology, Peter Millard
January 30, 2015 · Comments Off on Bi265j Mentioned in the Goldfarb Center Newsletter!
For the last two years the Goldfarb Center has generously supported a variety of activities in Bi265j Human Anatomy and Physiology through their Civic Engagement Course Development Grant. These activities include:
- A tour of Maine General Augusta and a presentation of their Grand Rounds talks along side similar talks from Human A&P students at Kents Hill prepatory HS to the third year UNE medical students on clinical rotations.
- Metabolic Analysis Lab in conjunction with the Waterville HS cross country team.
- Development of an internship for a former Bi265j student shadowing a nurse pratitioner in the Inland Hospital system in conjunction with being a TA for the Bi265j class.
- Bringing high school students interested in human A&P from a variety of regional school districts to campus for a day of mentoring by Bi265 students in collaboration with the Maine Math and Science Alliance. Activities included touring the anatomy lab, a hands-on pig heart dissection, and a brain storming session for helping the students develop human A&P based projects for the 2015 Maine State Science Fair.
These activities were recently mentioned in the latest Goldfarb Center newsletter which you can read here.
From myself and all of the Bi265j students at Colby and high school students from across the state that have benefited from the Goldfarb Center’s support, we give you our thanks. A special thanks to Alice Elliot, the Goldfarb Center’s Associate Director for her considerable logistical support and Amanda Cooley, the Assistant Director, for the write up in the GC newsletter.
Categories: Special Activities · Uncategorized
Tagged: Goldfarb Center
January 28, 2015 · Comments Off on Grand Rounds: Atypical Hyperplasia of the Breast
Ariel Oppong, Jay Lee, Rebecca Gray
http://youtu.be/_0jV_CS7gXo
Grand Rounds _Hyperplasia powerpoint pdf
Grand Rounds Synopsis- Atypical Hyperplasia of the Breast
Hyperplasia occurs when an organ or tissue becomes enlarged because the cells within it begin to proliferate more quickly than usual, resulting in an abnormally large population of cells in one, concentrated area of the body. We categorize hyperplasia in two ways: (1) “simple” or “complex”, and (2) “usual” or “atypical”. The research we will explore focuses on complex, atypical hyperplasia. This refers to hyperplastic tissue that both engorges the tissue around it and contains deformed, non-uniform cells.
Hyperplasia of the breast falls into two categories: lobular and ductal. Within the fatty tissue of a healthy breast are mammary glands, and within those lie lobular clusters of alveoli. The cuboidal cells that line these alveoli secrete milk, which moves through milk ducts to reach the nipple, where it is excreted during breastfeeding. When hyperplasia occurs in the breast, it is usually found in either the lobules of the mammary gland or the associated milk ducts.
Usually, hyperplasia within the breast is relatively harmless. Because change in breast size and shape occurs normally over the course of a woman’s life, her body is designed to handle minor engorgement of the tissue there. This condition becomes concerning when hyperplastic cells within the breast become atypical; this is characterized by misshapen cytosol, nuclei, and membrane organization. When this occurs, the hyperplastic cells take on characteristics startlingly similar to those of tumors: they are clumped, proliferating rapidly, and lacking functionality. For this reason, atypical hyperplasia of the breast is linked with breast cancer and considered premalignant.
Usually if a lump or an abnormal mass is found during a female’s mammogram then a health professional will usually suggest a biopsy. During the biopsy tissue cells are removed for analysis by a pathologist. If the pathologist can not make a definite decision as to if the excision is cancerous or not.
A 2014 report published by the New England Journal of Medicine published a new meta-analysis of the associated risk of breast cancer associated with atypical hyperplasia. The conclusions of the meta-analysis suggested that a women with a atypical hyperplasia has a least a 30% increased risk of having breast cancer within a 25 year follow-up. Due to this new information we ( the anatomy group) as well as the authors of this newly published report agree that there needs to be a reform in women’s health policies so that women are more aware of their risk and are also more informed about some preventative medicine including screening techniques, and treatment or surgical options if signs of breast cancer are already apparent.
Some of the current commonly used treatments are different types of SERMS. SERMS are selective estrogen receptor modulators. The most widely used antiestrogen for management of breast cancer is Tamoxifen. However, prolonged use of Tamoxifen does increase one’s risk for endometrial (uterine) cancer.
Another important issue is the health disparities in breast cancer diagnosis, quality of treatment, and mortality rates among different socio-economic groups, geographic locations, the unemployed and employed, and racial groups. Based of off data from the 2014 Racial Disparity in Breast Cancer Mortality Study in areas such as Memphis, Tennessee, black women are more than two times more likely to die of breast cancer than their white counterparts. Overall, our research indicates that we as a country need to implement new screening methods, need to promote more education initiatives, need to enact new policies to decrease health disparities, and need to stress the powerful conclusions that meta-analysis provide.
Categories: Grand Rounds
Tagged: Ariel Oppong, Jay Lee, Rebecca Gray
January 28, 2015 · Comments Off on Grand Rounds: Oligoastrocytoma
Grand Rounds: Oligoastrocytoma
Alex Lucas, Yvette Qu, Rachel Bird
http://youtu.be/wguUeUNttac
Grand Rounds_Oligoastrocytoma_powerpoint pdf
Oligoastrocytoma
Oligoastrocytomas are brain tumors that consist of oligodendrocytes and astrocytes, the two cell types in the brain that support and insulate nerve cells. Unlike many brain tumors, which typically present initially with headaches, seizures are a common initial symptom of oligoastrocytomas.
The patient presented with episodes of “a feeling of walking through a cloud,” receptive, or Wernicke’s aphasia (the inability to understand spoken words), Aphasia (inability to speak), and vertigo. She also suffered from brief seizures, which worsened in severity over the course of the next eight years, and began to involve loss of consciousness and muscle tone, occasional incontinence, and overwhelming confusion. Three months prior to admittance, the patient struck her head during an episode, but MRI, ECG, echocardiography, Holter monitoring, EEG and multiple blood tests all appeared normal. The patient did not respond to triptans or beta-blockers, but the frequency of her seizures increased to at least one per day.
An MRI was performed on the patient, which showed a mass in the left occipitotemporal region of the brain. A biopsy helped to determine the grade of the tumor – grade II, which is a low grade tumor – and also presents the pathology which helps to determine the growth patterns of the tumor cells. Fluorescence in situ hybridization (FISH), which allows for reliable and accurate detection of chromosomal deletions, showed deletions in 1p and 19q tumors.
Similar to most tumors, the exact cause of an oligoastrocytoma is unknown. It is understood that normal cells become abnormal in the sense that they may produce the wrong number of proteins or enzymes or be lacking certain genetic material. In the case of an oligoastrocytoma, deletions of genetic information in chromosomes 1p and 19q are the reason for the tumor cell’s abnormalities. This certain type of tumor is a result of a mixture of oligodendrocytes and astrocytes. Genetic material losses in 19q occur in 60-80% of oligodendrogliomas and 30-40% in astrocytomas, which demonstrate that there may be a shared variation in the formation of gliomas. Losses in the 1p chromosome are frequent with oligodendrogliomas at about 50-80%, however are less apparent with astrocytomas, which is detected only 10-18% of the time. However, the combination of genetic material losses of the 1p and 19q chromosomes is detected in 60-80% of oligoastrocytoma cases.
A gross resection was performed to remove the patient’s low-grade oligoastrocytoma tumor. Standard radiotherapy and antiepileptic medications were given after the resection. Lifelong MRI was suggested instead of permanent pacemaker due to the low-grade of the tumor. Following MRI shows only postsurgical changes, implying good prognosis. During the 24-month following the resection, no seizure has occurred with reduction in medication, indicating great possibility of freedom from seizure in 10 years and absence of intractability.
The patient’s case is complicated by ictal asystole (stopping of the heart during her epileptic seizures, which is very rare) in a patient with a predisposition to neurocardiogenic syncope (fainting, loss of consciousness, loss of muscle tone due to an abnormal control mechanism of the brain over the heart) due to a genetic disorder, and with the asystole being triggered by the seizures caused by her oligoastrocytoma make this case very interesting and unique. The important information the case conveys is that a patient’s symptoms are not always indications of a single disease, and sometimes the symptoms need to be closely examined and can suggest more than one disease. Perhaps screening for relationships between cardiac dysfunction and neurologic mechanisms could help identify rare cases such as this one, which would allow for earlier diagnosis and treatment.
References:
(1) Paleologos, N A, ed. Oligodendroglioma and Oligoastrocytoma. Am Br Tum Assoc 2014: 3-8.
(2) Oligoastrocytoma. Univ CO Sch of Med Neusrgy 2015.
(3) Meenakshi G, MD, Azita Djalilvand, MD, Daniel J. Brat, MD, PhD. Clarifying the Diffuse Gliomas. Am J Clin Pathol. 2005;124(5):755-768.
(4) Cole, AJ, M.D., Eskandar, E. M.D., Mela, T, M.D., Noebels, J.L. M.D., Ph.D., Gonzalez, R.G. M.D., Ph.D., McGuone, D, M.B., Ch.B. Case 18-2013 — A 32-Year-Old Woman with Recurrent Episodes of Altered Consciousness. N Engl J Med 2013; 368:2304-2312.
(5) Ucdenver.edu. Department of Neurosurgery [Internet]. 2015 [cited 2015 Jan 15]; Available from:http://www.ucdenver.edu/academics/colleges/medicalschool/departments/Neurosurgery/patientcare/multi-disciplinaryprograms/AdultBrainTumorProgram/Pages/Oligoastrocytoma.aspx
Categories: Grand Rounds
Tagged: Alex Lucas, Rachel Bird, Yvette Qu
January 28, 2015 · Comments Off on Grand Rounds: Postpartum Coronary Artery Dissection
Lauren Shirley, Allison O’Connor, Cal Robbins
Grand Rounds Synopsis
Case 28-2010 A 32-Year-Old, 3 Weeks Postpartum with Substernal Chest Pain
http://youtu.be/bODWv-x-eDc
Grand Rounds Case Presentation powerpoint pdf
Onset
A 32-year old woman had an uncomplicated, spontaneous vaginal delivery after 39 weeks of gestation. This was the patient’s second pregnancy. During her first pregnancy, she was diagnosed with preeclamptic toxemia which was treated with magnesium sulfate. Mild hypertension (systolic 120-140 mm Hg) was reported during the first and third trimesters of her second pregnancy followed by a return to normal blood pressure. Upon delivery, it was noted that her placenta weighed 340 g (below the fifth percentile for gestational age, mean 540 g) with increased amounts of perivillous fibrin (suggesting placental ischemia- lack of blood and thus oxygen and glucose to tissue).
The patient was admitted three weeks post partum when she developed pain in the left jaw and substernal area. The patient called EMS and was given oxygen which resolved her symptoms after 20 minutes and EMS personnel left. The pain returned shortly and EMS returned whereupon the pt scored her pain as a 7 out of 10. Blood pressure was noted as 148/74 and an electrocardiogram (ECG) revealed normal sinus rhythm of 90-100 bpm and ST-segment elevation of 4 mm in leads V2 and V3 (Abnormalities in ECG). Oxygen, acetyl-salicylic acid, nitroglycerin and morphine were administered. When examined at the hospital, the pt’s blood pressure was 143/92 mm Hg in her left arm and 137/81 mm Hg in her right arm with a pulse of 83-92 bpm.
Diagnosis
With a chief complaint of chest pain the patient could have been experiencing cardiovascular, pulmonary, gastrointestinal or musculoskeletal complications. Since the patient was 32 years old, cardiovascular complications would seem unlikely, however, since the patient was three weeks postpartum cardiovascular complications need to be considered more carefully since the risk of acute myocardial infarction is increased during pregnancy and the postpartum period and since pregnancy is a risk factor for aortic dissection. The risk of pulmonary embolism (a blockage of an artery in the lungs) is also increased during the postpartum period.
Since the patient’s ECG showed ST-segment elevation in conjunction with chest pain, an acute myocardial infarction would be suspected. Approximately 35% of postpartum women who present with myocardial infarction have a coronary artery dissection. There are two main types of coronary artery dissections, those that are caused by mechanical precipitation and those that are spontaneous. A spontaneous dissection is a tear in the artery where the tunica media and tunica externa separate, allowing blood to pool in between these layers. SCAD are rare, however 75% of patients who present with spontaneous aortic dissections are women and 30% of those women are peripartum, suggesting that this patient’s coronary artery dissection was spontaneous. There are four subgroups of spontaneous coronary artery dissections, however peripartum status and idiopathic spontaneous coronary-artery dissections or those caused by coronary shear stress are the two subgroups relevant to this case. Since the chest pain began after the patient picked up her toddler, there is a high index of suspicion that this dissection may have been caused by the patient’s peripartum status and coronary shear stress caused by lifting her toddler. Angiographic projections showed 35mm long segment of narrowing in the left anterior descending coronary artery. The lack of vascular disease in other coronary arteries along with the patient’s postpartum status as well as her test results are consistent with the diagnosis of a postpartum coronary-artery dissection.
Treatment Options
Unlike aortic dissections, the usual chest pain drugs (asprin, nitroglycerin, etc) which thin the blood can actually help, keeping the true lamen patent. Beta-blockers and nitrates are often used to prevent superimposed vapospasm. In cases of myocardial ischemia or compromised coronary flow, reperfusion therapy is used. In patients with severe ischemia, coronary-artery bypass grafting is done. In this case, the patient was given an intra aortic balloon pump which helps to increase myocardial oxygen supply by being placed in the aorta where it inflates and decreases based on the heart beat. Since the patient had no pain and the Percutaneous Coronary Intervention could have entered the false lumen, and since coronary dissections can heal by themselves, the balloon pump makes the most sense. This increased blood flow to the coronary artery. Aspirin as an antiplatelet, ß-blockers, and statins were used in case of intramural hematoma in the coronary vessel. Because of the potential for emergency cardiac surgery, the patient was not given glycoprotein IIb/IIIa inhibitors.
After 2 days a significant improvement was noted, the pump was terminated, and since surgery was now unlikely, glycoprotein inhibitors were initiated for a minor myocardial infarction discovered during treatment of the aortic dissection. This would be discontinued in a year, while aspirin was recommended indefinitely. The patient was able to return to her normal life with no further complications.
Little evidence exist in terms of the cause of spontaneous coronary artery dissections, but the current theory is that inflammation is caused by hormones, which explains the prevalence in post partum women. Several studies also included women taking oral contraceptives as being at risk for coronary artery dissections. The eosinophils release the histolytic agents between the tunica media and the tunica adventitia, which cause dissections in coronary arteries.
References
- Sabatine, Marc S., Farouc A. Jaffer, Paul N. Statts, and James R. Stone. “Case 28-2010: A 32-Year-Old Woman, 3 Weeks Post Partum, with Substernal Chest Pain.”The New England Journal of Medicine (2010): n. pag. Web.
- James, A. H. “Acute Myocardial Infarction in Pregnancy: A United States Population-Based Study.” Circulation 113.12 (2006): 1564-571. Web.
- Koul, Ashok K., Gerald Hollander, Norbert Moskovits, Robert Frankel, Leo Herrera, and Jacob Shani. “Coronary Artery Dissection during Pregnancy and the Postpartum Period: Two Case Reports and Review of Literature.” Catheterization and Cardiovascular Interventions 52.1 (2001): 88-94. Web.
- Mcintyre-Spatar, Leslie, and Kevin H. Silver. “Spontaneous Coronary Artery Dissection in a Postpartum Woman: Literature Review.” The Journal for Nurse Practitioners 7.9 (2011): 770-73.
- Oliveira Marta Silvia, Goncalves Alexandra, Dias Paula, Maciel Júlia Maria. “Spontaneous Coronary Artery Dissection: a Diagnosis to consider in Acute Coronary Artery Syndromes” Artigos de Revisão. (2009): 28 (6): 707-713
- Heart Assist Devices. Texas Heart Institute, 2015. (Accessed January 20, 2015 at http://www.texasheart.org/Research/Devices/iabp.cfm)
- CBC. MedlinePlus, 2015. (Accessed Janury 25, 2015 at http://www.nlm.nih.gov/medlineplus/ency/article/003642.htm)
- Placental Pathology. University of Chicago. (Accessed January 20, 2015 at https://pathology.uchicago.edu/sites/pathology.uchicago.edu/files/uploads/PDFs/Placental%20Pathology%20Notes%20Aspen%202014%20-Fritsch%20final.pdf)
- Electrolytes. AACC, 2013. (Accessed January 25, 2015 at http://labtestsonline.org/understanding/analytes/electrolytes/tab/test/)
- CK-MB. AACC, 2013. (Accessed January 25, 2015 at http://labtestsonline.org/understanding/analytes/ckmb/tab/sample/)
Categories: Grand Rounds
Tagged: Allison O’Connor, Cal Robbins, Lauren Shirley