January 29th, 2014 · Comments Off on Grand Rounds: Creutzfeldt-Jakob Disease – An 80-Year-Old Man with Fatigue, Unsteady Gait, and Confusion
By: Kasey Kirschner, Jenna Passaggio, Phoebe Hughes
http://youtu.be/8_y3yc_sFoM
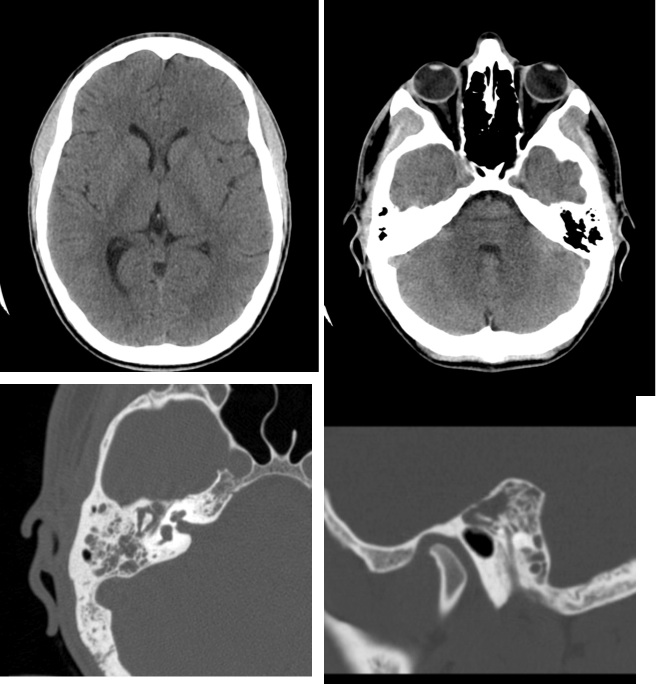
Four weeks before admission an eighty year old man presented with fatigue, insomnia, confusion, and difficulty walking. These symptoms may seem normal for elderly, but they were very uncharacteristic for him. As his symptoms worsened, he was admitted to the hospital. However, all tests conducted showed normal results. The test for 14-3-3 protein, which could indicate Creutzfeldt-Jakob, came back negative. An MRI showed loss of brain volume and changes in his white matter. He was given multiple drugs for insomnia, and he was released three days later. Cognitive abilities continued to decline, and he began experiencing tremors in his left arm and leg. He was readmitted to the hospital fifteen days later. Though many tests were done, all returned normal. Nevertheless, his symptoms continued to worsen, and he died after twenty third day of readmission.
The diagnosis was sporadic Creutzfeldt-Jakob disease with MM1. This diagnosis is most likely because of the rapid progression of the patient’s myoclonic jerking and dementia. Additionally, the patient presented with multiple symptoms consistent with other patients diagnosed with Creutzfeldt-Jakobs, including confusion, insomnia, and cerebral ataxia. Despite this, other tests which may indicate Creutzfeldt-Jakobs, such as an MRI or tests for the 14-3-3 protein did not confirm the diagnosis. Upon autopsy, a loss of neurons on the thalamus and spongiform changes of the cerebral cortex were found. This, combined with other symptoms, is indicative of sporadic Creutzfeldt-Jakob disease. However, the patient’s visit to England may suggest the variant form of Creutzfeldt-Jakobs. Only the brain was autopsied, and no other tissues were searched for presence of the PrPSc protein. The PRNP gene was sequenced and showed no mutations, which ruled out familial Creutzfeldt-Jakob disease. Ultimately, the final diagnosis was sporadic Creutzfeldt-Jakob disease.

Creutzfeldt-Jakob is hard to diagnose because there is no single test to confirm it, and the tests available can sometimes be misleading. There are a few which may help indicate the disease such as MRI’s, tests of the cerebrospinal fluid, and EEG’s. The presence of the 14-3-3 protein in the cerebrospinal fluid, high signal intensity on an MRI of T2 weighted images in the basal ganglia, or triphasic spikes on EEG can signify Creutzfeldt-Jakobs. In this case study, none of these tests showed signs of the disease. An autopsy of the brain and spinal cord may be done to see spongiform changes and neuronal loss.
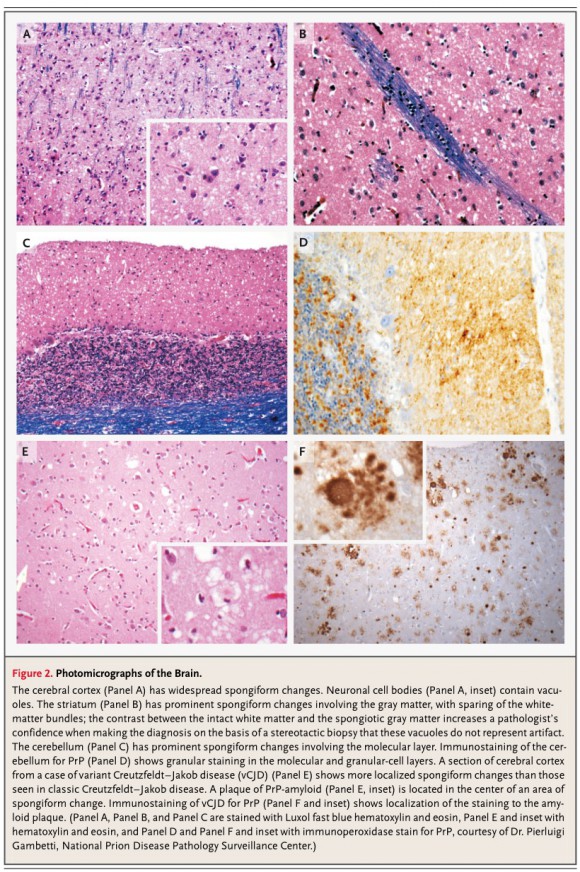
Creutzfeldt-Jakob disease is a rare disease affecting approximately one in a million people. It is caused by an infectious prion misfolding. This prion in its active state causes other proteins to misfold as well. Prions are resistant to proteinase K, which breaks down proteins. This makes them hard to destroy. It can be transmitted through transfusions or transplants. However, the sporadic form of Creutzfeldt-Jakobs disease causes the prions to misfold and become infectious spontaneously. The accumulation of misfolded prions causes holes in the brain which degenerate the brain matter. The neurodegeneration causes numerous and various problems in the patient.
Although some clinical trials are underway, no cure is currently available. Various treatments have been tested, and some patients have shown very brief periods of improvement, but nothing is available that stops CJD completely. This disease is treated by alleviating symptoms of the disease to make the patient more comfortable prior to death.
References:
1. “Creutzfeldt-Jakob Disease Fact Sheet.” National Institute of Neurological Disorders and Stroke. National Institutes of Health, 31 Dec 2013. Web. 12 Jan 2014. <http://www.ninds.nih.gov/disorders/cjd/detail_cjd.htm>.
2. Richard T. Johnson, M.D., R. Gilberto Gonzalez, M.D., and Matthew P. Frosch, M.D., Ph.D. Case 27-2005 — An 80-Year-Old Man with Fatigue, Unsteady Gait, and Confusion. N Engl J Med 2005; 353:1042-1050.September 8, 2005.DOI: 10.1056/NEJMcpc059024
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Grand Rounds: History and Advances in Kidney Transplantation
By: Kumba Seddu, Sophie Suechting, Blake McCartney
http://youtu.be/bgJ-zw1P40Y
As of June 21, 2013 96,645 people in the United States await kidney transplants. Last year, 4,903 patients died while awaiting a kidney transplant. These patients suffer from very advanced chronic kidney disease, which requires dialysis or a kidney transplant to maintain life. The two main causes of chronic kidney disease are diabetes and high blood pressure, which are responsible for up to two-thirds of the cases.
Experimentation with renal transplantation started in humans around 1906. There were many failed attempts using kidneys (and other organs) from animals; this method resulted in tissue rejection and was ultimately fatal. In 1954 Murray performed the first successful transplant with a donor on the identical Herrick twins – the kidney started producing urine immediately. Shortly after, in 1960, Murray performed another successful transplant on twelve year-old twins Johanna and Lana Nightingale. Murray was unable to perform advanced tissue and blood typing, but the transplants worked because the twins were an exact match. Later, advancements for non-twin donor pairs developed. Research also continued in the field of immunology, improving transplantation success rates and decreasing cases of tissue rejection.

Dr. Murray (left) and the Herrick twins.

Dr. Murray (center) and the Nightengale twins.
The kidneys are located in the back of the abdominal cavity in the retroperitoneum. Their function is to filter blood and remove waste from the body. If the kidneys are unable to adequately filter waste products from the blood, the body can enter renal failure. Renal failure requires regular dialysis or a kidney transplant to maintain proper bodily functions.
Scientists have always been fascinated with discovering a way to preserve organs for transplantation. It was discovered that there is a reversible effect of hypothermia on the metabolic processes of isolated tissues and that when the tissues are rewarmed their function returns to normal. There are currently two main methods of organ preservation that both freeze the tissues: machine perfusion and simple cold storage. Machine perfusion was researched first as it seemed to most effectively mimic the actual physiology of the organ. Cold storage was discovered soon after and became the primary method of organ storage due to its simplicity, quality of organ preservation, and cost effectiveness. There still remains a debate today as to which preservation method is best, but cold storage continues to be the method of choice due to its simplicity and a lack of clinical evidence advocating for machine perfusion instead.
Due to the increased rate of surgical morbidities, the diseased kidney is usually left in its position. The transplanted kidney is placed in a different position, usually the iliac fossa, using a different blood supply. The renal artery of the kidney, branching from the donor’s abdominal aorta is connected to the recipient’s external iliac artery. The renal vein initially connected to the donor’s inferior vena cava is joined to the recipient’s external iliac vein.

The optimization of the Paired Donor Schema helps to increase the degree of compatibility in recipient and donor antigens. Blood test, Tissue test and cross matching are done on both recipient and donor and the results are then computed into an algorithm from graph theory. A random permutation is done and compatible matches are identified. This reduces rejection and helps better the transplant procedure.

Sources:
“About Chronic Kidney Disease.” The National Kidney Foundation: Kidney Disease. N.p., n.d.
Web. 14 Jan. 2014. <http://www.kidney.org/kidneydisease/aboutckd.cfm>.
Moers, Cyril, Jacques Pirenne, Andreas Paul, and Rutger J. Ploeg. “Machine Perfusion or Cold
Storage in Deceased-Donor Kidney Transplantation.” The New England Journal of Medicine (2012): n. pag. Web. 15 Jan. 2014.
Petechuck, David. “Organ Transplantation .” Google Books. N.p., n.d. Web. 15 Jan. 2014.
<http://books.google.com/books?id=POQB4YIjAnoC>.
Smith, Rebecca. “Breakthrough in Kidney Transplant ‘could Cut Waiting List'” The Telegraph.
Telegraph Media Group, 30 June 2008. Web. 15 Jan. 2014.
Smith, Susan. “Immunologic Aspect of Organ Transplant.” Medscape Log In. N.p., n.d. Web. 15
Jan. 2014. <http://www.medscape.com/viewarticle/436533_11>.
Terasaki, Connolly, and Jeffrey L. Veale “The New England Journal of Medicine.” Kidney Paired
Donation. N.p., n.d. Web. 15 Jan. 2014. <http://www.nejm.org/doi/full/10.1056/NEJMc1106996>.
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Grand Rounds: Bath Salt Subtance Abuse – A 36-Year-Old Man with Agitation and Paranoia
By: Thomas Kader and Michael Chiu
http://youtu.be/-xVmKhkJuJw
Background
Our case study focused on the case of a 36 year old man who was rushed to the hospital after his girlfriend called EMT. He was initially reported to be running naked through the streets, tachycardic, was extremely agitated, paranoid, and lacked the ability to communicate. He also had a high body temperature and was diaphoretic. In terms of pertinent medical history, the man suffered from depression, and had just recently been laid off from his job. In addition, he had a history of alcohol and drug abuse, and was smoking tobacco at the time. He had no known allergies to medications but was but was lactose intolerant and allergic to shellfish. His family had a history of hypertension, coronary disease, and diabetes mellitus. His only medication was fluoxetine, an antidepressant, which he hadn’t taken for 2 weeks. He also had taken bath salts intranasally for the prior 3 days. Initially, the patient was given midazolam and Lorazepam via IV, intubated for airway protection, and sedated with Propofol. A CT scan was taken with no acute pathology. The patient was then transported to the ICU, where he was given benzodiazepines and neuroleptics, as well as endotracheal intubation.

Commercially available methcathinone “bath salts”

Man chewing khat leaves, a naturally occurring source of cathinone.
Differential Diagnosis
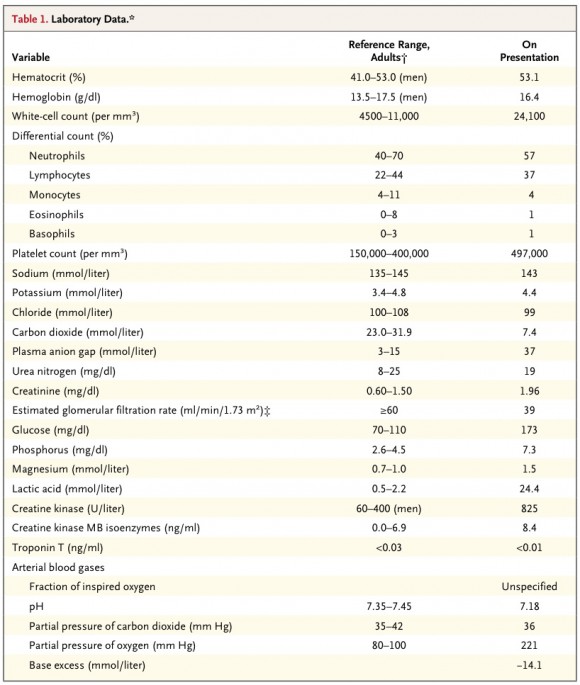
A clinical differential diagnosis was then conducted with clinical presentation showing: agitated delirium, aggressive violent behavior, hallucinations, paranoia, possible seizure, mydriasis, tachycardia, hypertension, and tachypnea, and diaphoresis. The diagnosis could either be toxic/metabolic, infectious, psychiatric, traumatic, or hemorrhagic/ischemic. It was determined that the symptoms most likely showed a toxic/metabolic cause because the patient had ingested a “bath salt” drug and was showing symptoms related to a toxic cause. For a toxic cause, there are many possible toxidromes that can be caused by different types of toxins. These toxins include anticholinergics, sympathomimetics, analgesics, toxic alcohols. Other possible toxidromes are sedative/hypnotic withdrawal, hemoglobinopathies, and serotonin syndrome or neuroleptic malignant syndrome. Doctors narrowed down the diagnosis to be caused by a sympathoimetic toxidrome, which is caused by ingestion of amphetamines, cocaine, or other sympathomimetics. Common symptoms associated with sympathomimetic toxidromes are hypertension, tachycardia, psychomotor agitation, diaphoresis, mydriasis, psychotic behavior, seizures, and coronary ischemia. It was known that the patient had ingested bath salts, which is a sympathomimetic toxin. The symptoms the patient was presenting also corresponded with the symptoms associated with those who have a sympathomimetic toxidrome. An initial CBC, or complete blood count test/blood panel test was conducted. The concentration of lactic acid in the patient’s blood was extremely high and the pH was very low. There was also a high concentration of creatinine and creatine kinase. These results suggested that the patient had metabolic acidosis, or high levels of acidity in the body, as well as rhabdomyolysis, or breakdown of skeletal muscle that can cause renal failure. The final diagnosis was acute ingestion of a synthetic cathinoine (Bath Salts) causing a sympathomimetic toxidrome with psychotic features and an acute lactic acidosis with acute renal failure.
Diagnostic Procedures
A serum test, a blood test using blood plasma with fibrinogens removed, using liquid chromatography with photodiode array detection (LC-PDA) was conducted, and it was positive for Lorazepam, Fluoxetine, Norfluoxetine, and Methcathinone. It was negative for common stimulants such as amphetamines and cocaine. A urine test using class-specific immunoassays was also conducted and was positive for amphetamines and benzodiazepines. The positive reading for amphetamine, however, was a false positive reading caused by Methcathinone cross-reacting in the amphetamine immunoassay conducted.
Treatment
The patient showed symptoms of cathinone toxicity: agitation, hyperthermia, metabolic acidosis, hyperthermia, rhabdomyolysis, tachycardia, hypertension, renal dysfunction, and oxidation by reactive oxidation species. To address these symptoms, GABA agonists as well as α-agonists were given to sedate the patient, and dopamine antagonists were given to attempt to reverse psychotic symptoms. To treat hypertension, the drug needed to be expelled. In addition, standard cooling measures were used and mechanical ventilation through endotracheal intubation was applied.
Mechanisms of disease
Based on the presented symptoms, doctors determined that the patient was undergoing malignant catatonia induced by Serotonin syndrome as well as Excited Delirium syndrome. Malignant catatonia is a variant of catatonia that is characterized by autonomic instability consisting of fever, tachycardia, and hypertension and is associated with psychiatric illness and drug ingestion. Serotonin syndrome is characterized by mental-status changes, autonomic hyperactivity, and neuromuscular abnormalities. Excited Delirium Syndrome is characterized by delirium, agitation, acidosis, and hyperadrenergic autonomic dysfunction, and is typically seen in drug abuse or mental illness. Serotonin syndrome occurs when there is an excess activity of serotonin at the serotonergic receptors of central and peripheral nervous systems. Excess serotonergic activity may be due to a combination of monoamine oxidase inhibitors and serotonin selective reuptake inhibitors, which prevent breakdown and reuptake of monoamine neurotransmitters including serotonin.
References
Benzer TI, Nejad SH, Flood JA, et al. Case 40-2013: A 36-Year-Old Man with Agitation and Paranoia. N Engl J Med 103; 369;26.
Singerman, Burton; Raheja, Ram. Malignant Catatonia: A Continuing Reality. Annals of Clinical Psychiatry. Vol 6(4), 259-266. http://psycnet.apa.org/psycinfo/1995-43892-001
Sporer KA. The Serotonin syndrome. Implicated drugs, pathophysiology, and management. US Library of Medicine, National Institutes of Health. Drug Saf. 1995 Aug;13(2):94-104.http://www.ncbi.nlm.nih.gov/pubmed/7576268
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Grand Rounds: Adolescent Stroke
By: Breanna Davis, Emmie Lai, and Adam Lavertu
http://youtu.be/p3D2P-WveNU
Rather than focusing on the specific case, we intend to discuss the incidence of ischemic strokes in adolescents drawing support from the case worked on by Phoebe H. Yager, M.D., Aneesh B. Singhal, M.D., and Raul G. Nogueira, M.D. Strokes in young adults are frequently misdiagnosed or not even recognized.
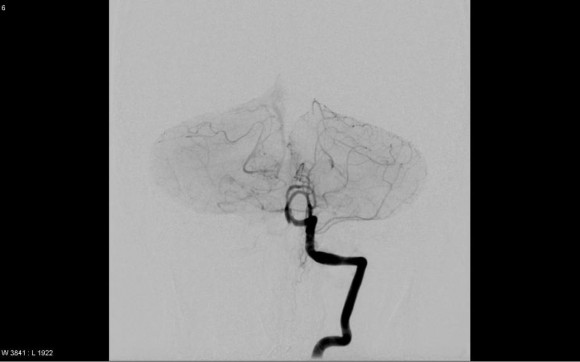
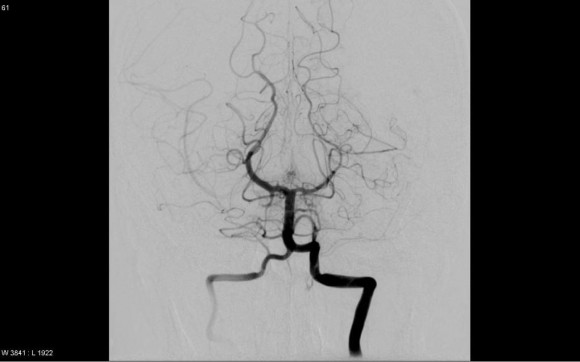
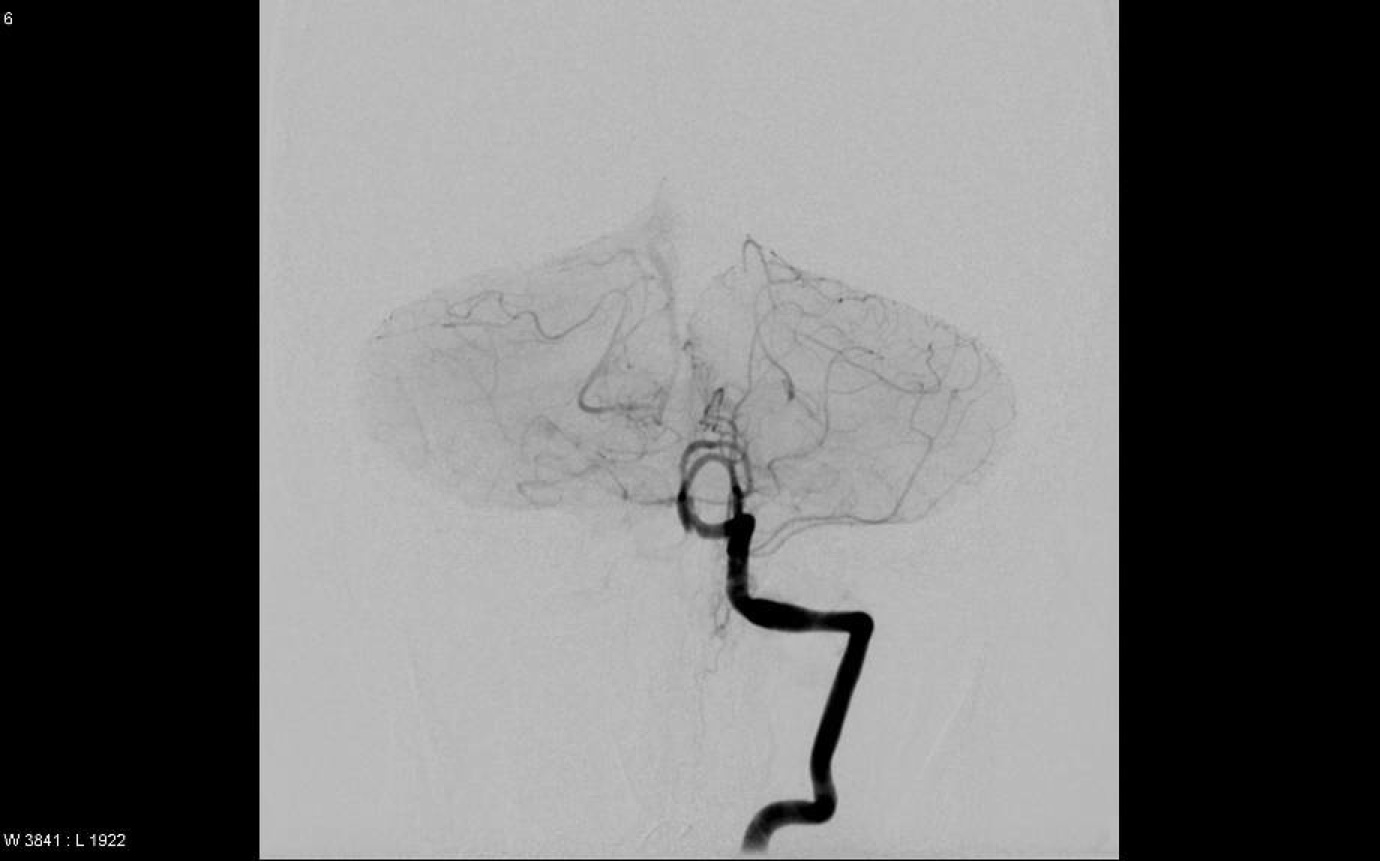
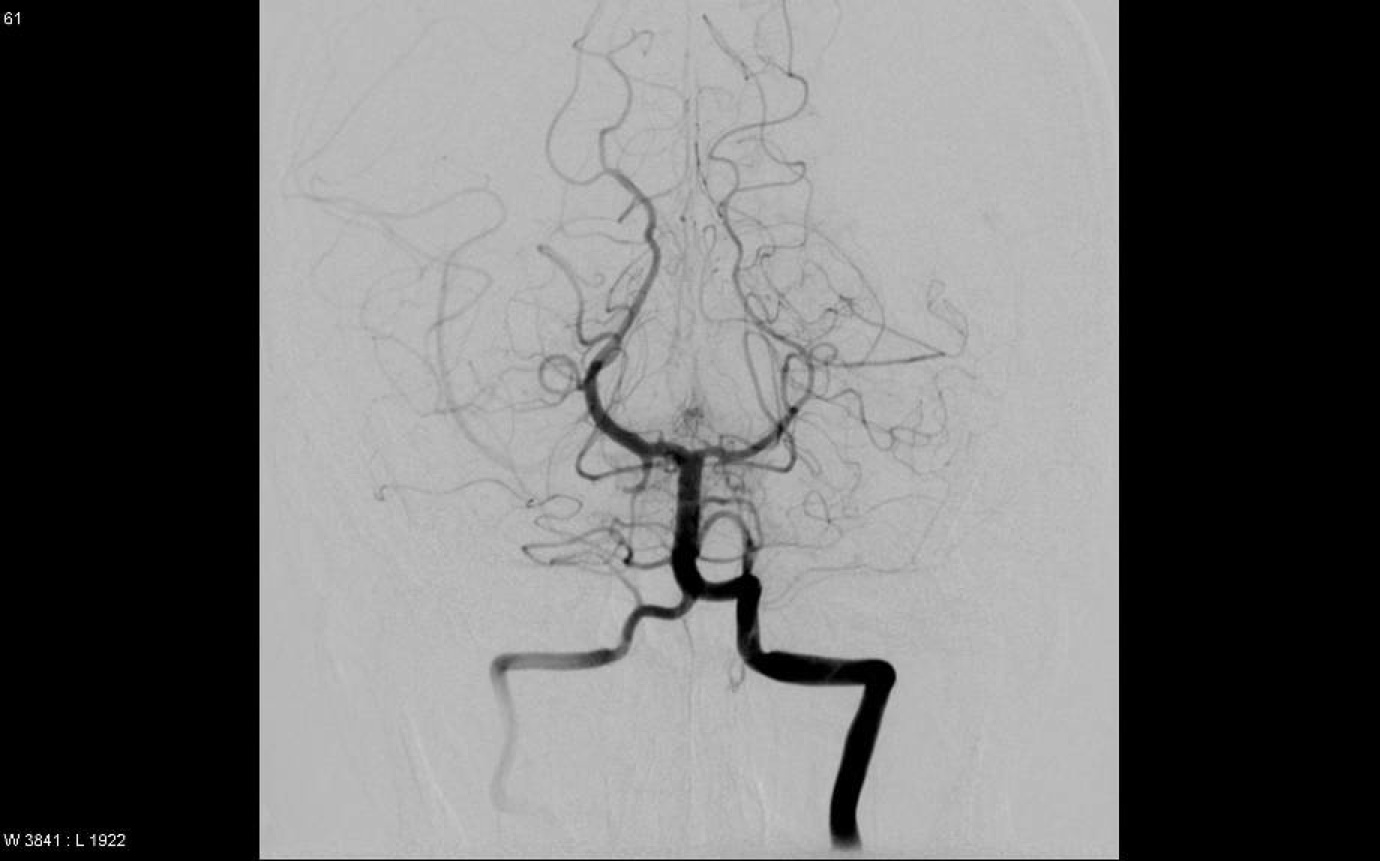
Pretreatment (above) and posttreatment (below) angiography
An ischemic stroke results from a blockage of a blood vessel that supplies the brain. This lack of blood results in oxygen deprivation of the brain; this is what we know as a stroke. There are two main types, cerebral thrombosis and embolisms. Thromboses are formed at the site of the blockage and while embolisms originate somewhere else in the body and travel to the site of the blockage. Some identifying risk factors of stroke include hypertension, diabetes and lipid issues. Many other diseases and conditions can also increase the risk of stroke, for instance patent foramen ovales (PFO) have a high correlation with strokes.
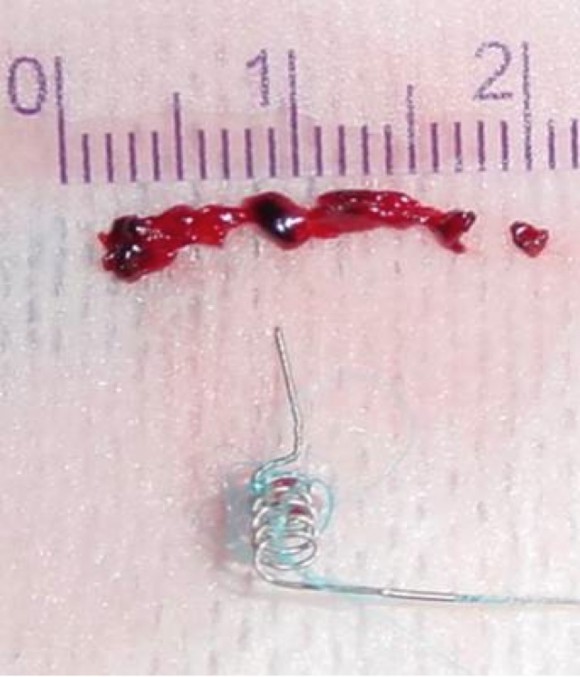
Retrieved thrombus and MERSI retriever.
PFOs result from a failure of the neonatal hole in the heart between the right and left atrium to close post birth. Normally the closure of which results in what we know as the fossa ovalis. PFOs can allow clots to enter the aorta, where the clot has the potential to travel to the brain possibly resulting in ischemic strokes. A surprising 14% of all strokes occur in children and young adults (Yager et al.). The majority of which are ischemic strokes, with a lesser incidence of hemorrhagic strokes.
There are over 18 Cardiac causes of stroke in young adults. However, of all these causes of cardiac strokes in young adults, 37% of the patients have a PFO. Unlike many of the causes, PFO’s are source of low and uncertain risk because just having a PFO doesn’t directly relate to a person having a stroke, since 1 in 5 Americans have PFO’s and many of these people go through life with no cardiac issues. Along with a PFO, a person has to have clot form in their blood, and their blood pressure must be high in the right atrium to build enough pressure to push open the flap and send the clot through to the left atrium. This is relevant to our case because our patient had a PFO and got it closed and had no further issues with ischemic strokes. He has made a full recovery but did come very close to death due to the late diagnosis. This was not a surprise because people under 50 are often misdiagnosed since the general public and clinicians are unaware of how often young adults do have strokes and it is not their first assumption.
Common signs are numbness in face or extremities, trouble speaking, disturbed vision, trouble with motor control, dizziness, and headache. Our patient presented with ataxia or impaired motor control, blurred vision, and dysarthria or slurred speech. Initially receiving clinicians searched for a tumor and other sources due to the young age of the patient. After, the rapid onset of symptoms they began to search for other causes. Within 20 minutes of admission to the original receiving hospital, the patient progressed from difficulty walking to needing a wheelchair, within hours he entered into a coma and was promptly transferred to Mass General via airlift. Doctors at Mass General made the correct diagnosis of stroke after performing diagnostic tests including CT scans and MRIs, because the patient was diagnosed with a stroke past the three hour window, he was treated with an endovascular reperfusion, or a minimally invasive clot retrieval surgery. The other options were both made use of pharmacological agents and ran the risk of cerebral hemorrhage. This is due to the possible malignant interaction between the drug and the infarcted tissue surrounding the occlusion. A Merci retriever was guided into the femoral artery to the location of the clot. The retrieved thrombus was 1.8 cm in length. The patient made a full recovery and his PFO closed after a year. He now lives a normal life with an aspirin regimen.
Through this case study, we hope to raise clinician awareness of the rate of strokes in young adults. As clinicians become more aware hopefully there won’t be as many late and misdiagnoses that lead to fewer treatment options, higher risk of fatality and increased treatment costs. Incidence of strokes in people under 34 has increased in recent years, particularly in males. Therefore, it is important that clinicians become more aware and have better clinical cues in order to more quickly work up to the stroke diagnosis, as this problem will only increase.
Works cited:
George MG, Tong X, Kuklina EV, Labarthe DR. Trends in stroke hospitalizations and associated risk factors among children and young adults, 1995-2008. Ann Neurol2011;70:713-721. http://www.ncbi.nlm.nih.gov/pubmed/21898534?dopt=Abstract. Accessed 13 Jan 2014.
“Ischemic Strokes (Clots).” Ischemic Strokes (Clots). American Heart Association, American Stroke Association. N.p., n.d. Webhttp://www.strokeassociation.org/STROKEORG/AboutStroke/TypesofStroke/IschemicClots/Ischemic-Strokes-Clots_UCM_310939_Article.jsp. Accessed 18 Jan. 2014.
Ji R, Schwamm LH, Muhammad P, Singhal AB. “Ischemic stroke and TIA in young adults: risk factors, diagnostic yield, neuroimaging and thrombolysis. Arch Neurol (in press).” JAMA Neurol. 2013 Jan;70(1):51-7. http://www.ncbi.nlm.nih.gov/pubmed/23108720. Accessed 14 Jan 2014.
Krasuski, R. M.D., Tuzcu, M. M.D., Kapadia, S., M.D. “Disease and conditions: Patent Foramen Ovale.” Clevelandclinic.org. Jan 2012. http://my.clevelandclinic.org/heart/disorders/congenital/pfo.aspx. Accessed 14 Jan 2014.
Yager, P.H., M.D., Singhal A.B., M.D., Nogueira, RG, M.D. “Case 31-2012: A Young Man with Neurologic Symptoms”. New England Journal of Medicine 368:2, 193-194. http://www.nejm.org/doi/full/10.1056/NEJMcpc1208150. Accessed 8 Jan 2014.
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Grand Rounds: 49-Year-Old Male with Adenocarcinoma of the Rectum and Novel Bacterial Therapy
By: Cameron, Lizzy, & Cody
http://youtu.be/F9ytiGVbKxs
Adenocarcinoma is cancerous disease that originates in mucus-secreting glandular tissues, most commonly in the lungs, pancreas, prostate, esophagus, colon/rectum. 95% of all colorectal cancers (CRC) are adenocarcinomas. Three months prior to diagnosis, the patient (Male, 49 years) notes blood in his stool. He went to his primary physician who found his physical examination to be normal. His father had colonic polyps, and his paternal grandmother had colon cancer in her 80s. Although family history of CRC is most significant in first degree family members, his father’s history of polyps may suggest a hereditary CRC predisposition in the patient. Six weeks before the patient’s presentation at MGH, he noted decreased stool caliber, and prolonged presence of blood and mucus in his feces. He went to see a gastroenterologist who performed a colonoscopy and discovered an exophytic mass 15 cm from the anal verge and 2 polyps in the descending colon.

At higher magnification, small infiltrating glands in desmoplastic stroma are diagnostic of moderately differentiated adenocarcinoma. The depth of invasion cannot be assessed from this small biopsy specimen.
Biopsy of the mass revealed dense stroma covered by villiform dysplastic epithelium, with stromal hypertrophy and small infiltrating glands, a characteristic that is indicative of moderately-differentiated adenocarcinoma. An axial CT image of the abdomen/pelvis revealed a rectal mass causing abrupt narrowing of the rectal lumen (3.2×3.1×6.8 cm). An MRI image showed the rectal mass extending through the muscularis propria and into the outer layer (serosa) of the colon. Ultrasonography-guided fine-needle aspiration and core biopsy of the inguinal lymph node determined that the cancer had not spread into the lymph node and was still limited to the colon (although locally advanced). Final diagnosis of the case was moderately differentiated, invasive rectal adenocarcinoma (Stage IIA).
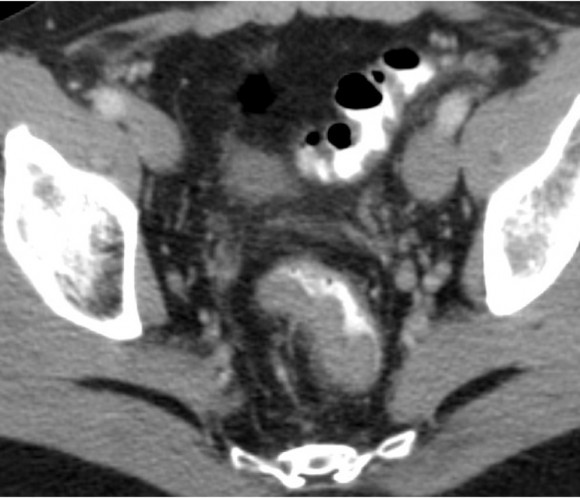
An axial image from the CT study with oral and intravenous contrast material that was performed at the other hospital shows a soft-tissue density in the rectum causing abrupt narrowing of the rectal lumen
The patient’s rectal cancer is advanced, and as such the first major treatment decision is whether to resect immediately or use preoperative (neoadjuvant) chemotherapy, radiation, and/or postoperative chemoradiation. The team of doctors recommended preoperative chemoradiation therapy with fluorouracil and radiation therapy. Stage I rectal cancer is often successfully treated with resection, but advanced rectal cancer cases such as Stage II or III typically need multiple treatment modalities (e.g. radiation). Lynch syndrome is an autosomal dominant disorder, and in this case is likely the cause of his colorectal cancer. According to the Amsterdam criteria, this patient did not qualify as having lynch syndrome. However, the Bethesda guidelines, which are more sensitive to subtle cases of Lynch syndrome, did suggest Lynch syndrome. Between 50 and 70% of people with Lynch Syndrome develop colon cancer in their lifetime, and the risk of syndrome is 50% to immediate family members–making clinical diagnosis important not only for the patient but for immediate family members as well. Postoperative treatment was complicated by a Superficial femoral-vein thrombosis which was treated with a 6 month course of heparin. The take down of his ileostomy was successful, with colon function being restored. He is now alive without recurrence more than 4 years after resection, and undergoes annual endoscopic surveillance and visits his doctor biannually.
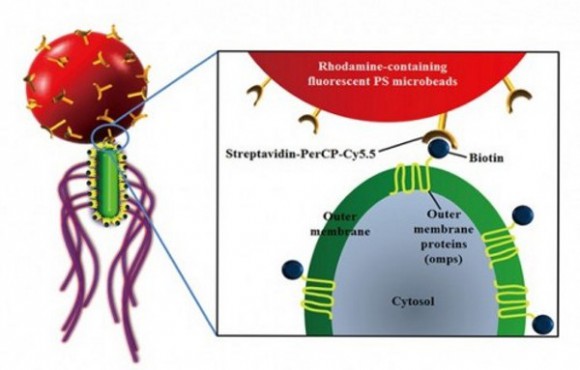
Scientists at Chonnam National University in South Korea have developed a way to selectively attach flagellar bacteria to polystyrene microbeads. The team modified Salmonella typhimurium with a selectively BSA (bovine serum albumin) pattered PS (polystyrene) microbead. S. typhimurium has been shown to aggregate around quiescent or necrotic tumors due to chemoattraction to tumor cell lysates and spheroids. The attached microbead can release the therapeutic compound inside of the tumor. The bacteria are also useful in detecting metastases and small tumors. One of the most significant challenges of chemotherapeutic treatments is the continuous, specific delivery of optimal quantities of drugs to target cells – which would allow the bacteriobot to shine in efficiency and selectivity of drug delivery. The advancement of this treatment could mean that a total colectomy may not be necessary if the cancer recurs in the colon. The treatment also could help eliminate the negative gastrointestinal issues associated with chemotherapy by reducing general cytotoxicity and negative body response to treatment.
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Ground Rounds: The Relationship Between Coronary Heart Disease and Childhood Obesity
By: Amanda Millatt, Michelle Daigle
http://youtu.be/E9-yFGlhJks
Coronary vasculature carry oxygen rich blood to the heart muscle and removes oxygen depleted blood. The left and the right artery each supply blood to a different part of the heart. Atherosclerosis is a disease that causes plaque to build up in arteries. Plaque is a buildup that consists of fat, cholesterol, calcium and other substances that can be found in blood. This plaque buildup can harden and narrow the arteries over the years, which limits the blood flow of oxygen-rich blood organs and other parts of the body. Atherosclerosis in the coronary arteries can completely block the flow of blood to the heart in some places or in others form a blood clot. This lack of blood to the heart tissues caused by a plaque buildup will cause the heart muscle to die, thus causing a heart attack. The blockage of blood flow can cause angina, a symptom that simulates a discomfortable pressure in the chest area and sometimes can extend to other part of the body.
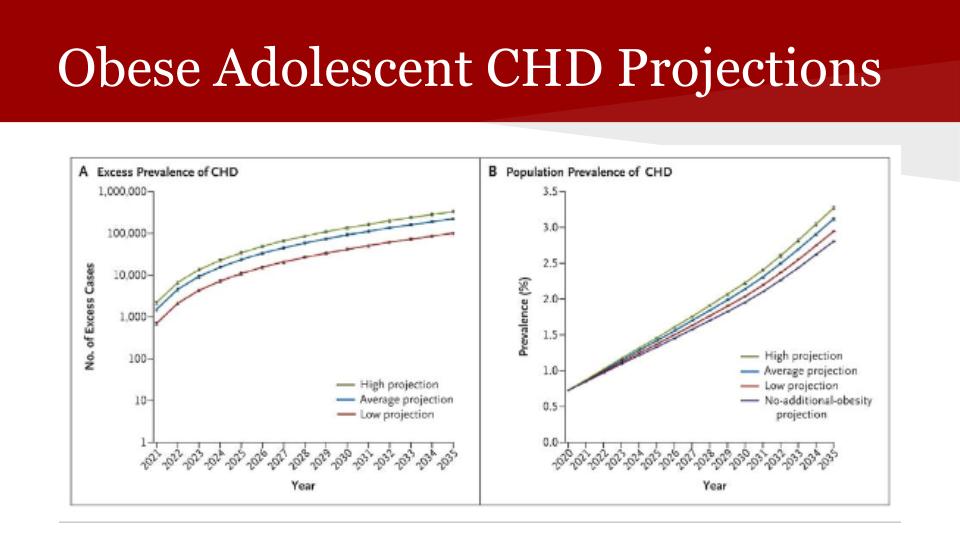
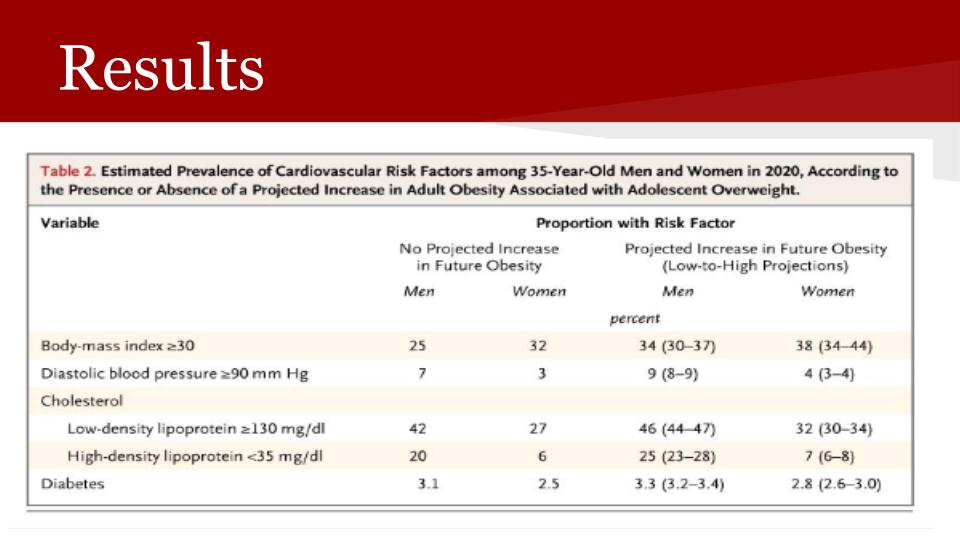
A study published in the New England Journal of Medicine examined the effects of adolescent obesity on coronary heart disease in adults for the projected year 2020. Through a series of studies relying on the U.S. census, the National Hospital Discharge Survey and a few other studies along with computer programs they were able to project the percentage of overweight adolescents who will develop coronary heart disease as adults. Having an elevated Body Mass Index (BMI), a calculation of your height and weight to determine weight classes, creates many different risk factors for coronary heart disease, which include hypertension, dyslipidemia, and diabetes. To run this study researchers used the parameters of adult obesity being defined as a BMI of 30 or more and adolescent obesity as being in the 95th percentile on the growth charts. From this study done in 2000, researchers predicted that for the year 2020 the obesity rate for men and women is supposed to increase significantly. This elevates the risk of coronary heart disease by increasing the risk for plaque buildup in the blood, elevating diastolic blood pressure, cholesterol buildup in the blood and the risk for diabetes. They also projected future obesity cases leading to coronary heart disease for the year 2035 and determined that the incidences of Coronary Heart Disease is expected to surpass 100,000 events for both their low, high, and average projections. Along these same lines they determined that through the use of treatment for high blood pressure and high cholesterol the rates of coronary heart disease due to obesity could be lowered.

Obesity has recently become prevalent in America because the increasing amount of sucrose in modern diets without fiber. Sucrose consist of glucose and fructose. America’s consumption of fructose went from 15g per day to now 75g per day. The explanation for obesity starts with the increase of fructose which causes the pancreas to produce more insulin, hormone that signal cells to take sugar from the blood. Simultaneously glucose is metabolized by the whole body and stored as glycogen. Fructose can only be metabolized by the liver, however the body produced enough glycogen to suffice. Thus the liver converts the fructose into fat. The carbohydrates from the food consumed floods the tissues instantly turning into fat. This fat sends a hormone called leptin to the hypothalamus to tell the body to stop eating. The leptin is not received by the hypothalamus because the access insulin blocks the leptin. Thus causing the brain to think that the body needs more energy and the person continues eating.
Strategies to reduce childhood obesity are eat more fiber, reduce consumption of sugary drinks, wait 20 minute for a second plate of food and physical activity. The increase fiber consumption will cause a decrease in blood sugar level if three or more grams are consumed. The reduction of sugary drinks such as soda or orange juice, will decrease the amount of insulin produced. Food after being consumed will take 20 minutes to move completely through the intestine. At the end of the intestine is where hormones are produced to signal the brain that the stomach is full. Physical activity will reduce stress and stress induced eating. Through these lifestyle changes the adolescent will be decrease their risk for coronary heart disease. 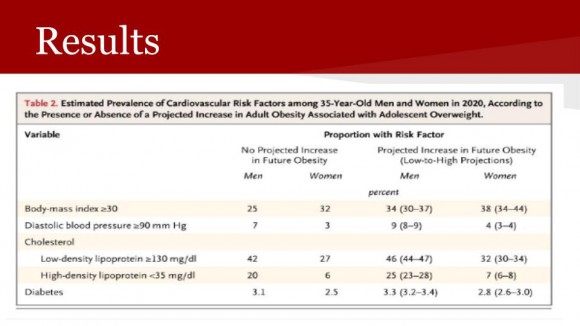
Resources
1. Anatomy and Function of the Coronary Arteries. Stanford Hospital, 2014. (Accessed January 12, 2013, at http://stanfordhospital.org/healthLib/greystone/heartCenter/heartIllustrations/anatomyandFunctionoftheCoronaryArteries.html.)
2. Bibbins-Domingo K, Coxson P, Lightwood J, Goldman L. Adolescent Overweight and Future Adult Coronary Heart Disease. N Engl J Med 2007; 357:2371-2379.
3. The Complete Skinny on Obesity. Perf. Dr. Robert Lustig. YouTube. YouTube, 23 Oct. 2013. Web. 28 Jan. 2014.
4. What is Coronary Heart Disease?.National Heart, Lung and Blood Institute, 2012. (Accessed January 12, 2013, at http://www.nhlbi.nih.gov/health/health-topics/topics/cad/.)
Tags: Grand Rounds
January 29th, 2014 · Comments Off on Grand Rounds: Epstein-Barr Virus and Infectious Mononucleosis Induced Acute Post-infectious Cerebellar Ataxia
By: Laurel W, Emma R, Peter W
http://youtu.be/iHSMb2sa8Dk
One month before admission to Massachusetts General Hospital, a previously healthy 19 year old male presented with fatigue, fever, pharyngitis, and lymphadenopathy. A streptococcal pharyngitis (strep throat) test was found to be negative, and a heterophile antibody test (rapid test for mononucleosis) was found to be positive. The diagnosis of infectious mononucleosis due to Epstein-Barr virus (EBV) was made 17 days before admission.
Two weeks prior to admission, the patient presented with additional symptoms, including dysphagia and pain and difficulty hearing in the right ear. A diagnosis of otitis media was made and was treated with prednisone, amoxicillin, and azithromycin. 8 days prior to admission, the patient presented with severe ear pain, a perforated right tympanic membrane, and a bloody purulent in the external auditory meatus. The patient was treated with oral cefurozime and ciprofloxacin (antibiotics). Several days after visiting the ENT, the patient returned for a myringotomy (procedure to relieve pressure in ear by making incision in ear drum). Then, 6 days prior to admission, the patient experienced unsteadiness, slurred speech, and increasing gait imbalance.
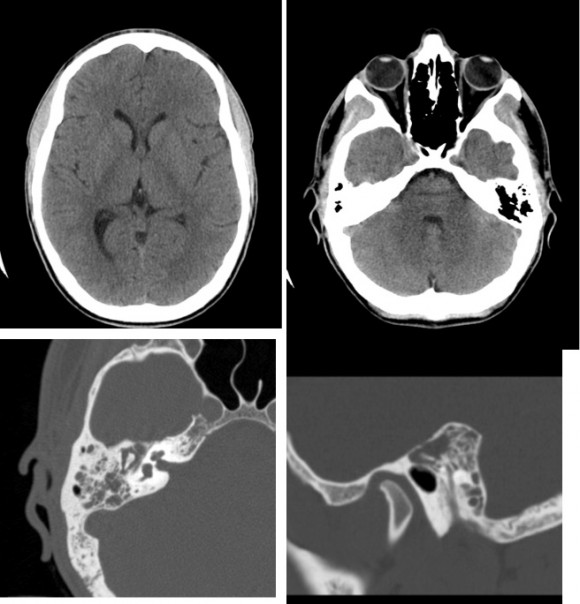
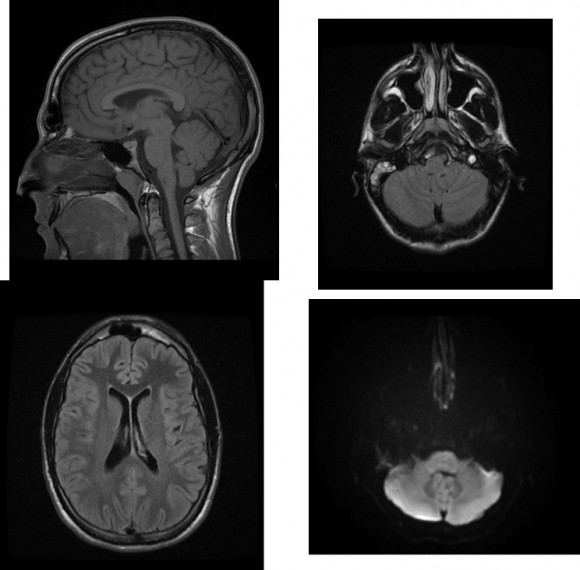
Upon arrival the patient had experienced weight loss, decreased hearing, enlarged tonsils, falling, and truncal ataxia. Over the first four days of admission the patient was found to have opacification (indicating fluid in these areas) of right mastoid air cells and middle ear (as shown from MRI and CT scans), impaired ability to perform simple arithmetic, continued deterioration of speech, and balance. The CT scans of the cerebrum and cerebellum showed no abnormalities. The coordination test showed impairment in his motor functions. Slurred speech, clumsiness, ataxia (lack of coordination of movements) and otitis media led to the admission of the patient to neurology services.
Although Guillian-Barre syndrome is the most common cause of post-infectious ataxia, it is accompanied by loss of reflexes, which were intact in this case. Although cerebral involvement due to executive dysfunction was considered, it could not explain all of the patient’s signs and symptoms. Hereditary and neurodegenerative diseases were ruled out due to lack of family history, normal imaging, and patient’s age. However, the patient’s symptoms, along with the diagnoses of infectious mononucleosis, led to the clinical diagnoses of an upper respiratory tract infection complicated by otitis media. The neurological symptoms also led to the diagnoses of post-infectious acute cerebellar ataxia (ACA) associated with Epstein-Barr virus. ACA is presumed to be an auto-immune response causing inflammation of the cerebellum leading to motor dysfunction.
Plasmapheresis and intravenous immunoglobulin (IVIG) were recommended for treatment as this course is directed at the immune response and therefore more effective. IVIG is administering a solution containing antibodies from the plasma of thousands of people and Plasmapheresis is the process of removing, treating, and returning blood plasma to a patient. Both techniques are common treatments for autoimmune disorders. On the fourth day in Massachusetts General Hospital a five day course of IVIG was begun; the patient responded rapidly and his symptoms improved. After the fifth day of treatment the patient had recovered 90% of his function. He then spent one day in a rehabilitation center and was discharged on the eighth day after admission with a full recovery.
Tracey A. Cho, M.D., Jeremy D. Schmahmann, M.D., and Mary E. Cunnane, M.D., et al. A 19-Year-Old Man with Otalgia, Slurred Speech, and Ataxia. N Engl J Med 2013;369:1253-1261
Tags: Grand Rounds